Eight phases of CHAPS
- CHAPS tools and templates to help get you started.
- Recommended steps.
- Links to supplementary materials and helpful websites.
CHAPS Quick Links:
- View local CHAs and PHIPs
- View local priorities over the years
- Explore the Colorado Health Indicators Dashboard
- Submit your CHA and CHIP here
Follow assessment and planning requirements
Download the Colorado Assessment and Planning Requirements Checklist.
Take a health equity approach
Using a health equity approach in your assessment and planning is essential to carrying out an impactful and meaningful process. We recommend general health equity resources and encourage you to apply this approach to best meet the needs of your communities and seek out the resources that you need to advance this approach.
On this page
| Phase 1 | Plan the process |
| Phase 2 | Equity and community engagement |
| Phase 3 | Conduct a community health assessment |
| Phase 4 | Assess capacity |
| Phase 5 | Prioritize issues |
| Phase 6 | Develop a plan |
| Phase 7 | Implement, promote, and monitor |
| Phase 8 | Participate in statewide public health improvement opportunities |
Include environmental health
The Colorado Public Health Act includes the field of environmental health under the broad definition of public health; therefore, environmental health service capacity and environmental and health outcomes should be documented during local assessment processes.
Optimize a regional partnership approach
Local public health agencies may consider taking a regional partnership approach to CHAPS. This approach can help build core public health service capacity in a region and throughout the state by better using scarce resources for assessment and planning activities. Any combination of the phases and steps can be conducted together or separately. At a minimum, it will be helpful to start this process during the same time frame to inform each other, particularly with the number of shared services and regional partners.
View the CHAPS status map to see how LPHAs are currently partnering.
Align with other assessment processes
The following are some examples of other assessment and plans to consider when planning and conducting CHAPS:
- Non-profit hospital community health needs assessments (CHNAs) are required by the Patient Protection and Affordable Care Act every three years to maintain their preferred tax-exempt status. Many LPHAs partner with their local hospitals to share data collection processes and results as well as to partner on shared priority issues.
- Other funders, including CDPHE programs, may also require an assessment to meet contractual requirements, such as the Communities Organizing for Prevention youth substance use prevention program.
- Each agency receives CDPHE Maternal and Childhood Health grants, many of which leverage the CHAPS process to meet their Maternal and Childhood Health goals.
This list is not all-inclusive. It is important to do a scan of other assessment and planning processes going on within your agency and community when beginning the CHAPS process.
Phase 1: Plan the process
Use this phase to help determine the project's scope; leadership, advisory roles, and relationships; develop partnerships; needed resources; timeline; and initial communications.
These planning steps are recommended and can be done simultaneously or in an order that makes the most sense for your agency and partners. Review all CHAPS phases before returning to Phase 1 to begin your planning. Timing, funding, and capacity assets can help drive how the assessment and planning process is initiated.
Timeline
Local and state public health agencies are required to carry out this process on a five-year cycle.
It's recommended that local assessments, prioritization, and, if possible, completed plans be submitted prior to each statewide plan to inform the development and implementation of the state plan. The next state health assessment is due in 2024 and the next state plan is due in 2025.
We recognize that not all Local Public Health Agencies are on the same timeline, so if you have any questions about when your next plan is due, reach out to us at ophp@state.co.us.
OPHP CHAPS tools and templates:
- Colorado Assessment and Planning Requirements Checklist
- Local CHA and PHIP Requirements, Public Health Act & PHAB 2022 Crosswalk
- CHAPS Budget Template
- Sample CHAPS Health Planner Position Description
- Sample CHAPS Project Manager Position Description
- Sample CHAPS Facilitator Position Description
- CHAPS Work Plan Template
Additional and external tools and guidance:
| PDFs: | Websites: |
| Public Health 3.0 | BARHII Framework |
| Healthy People 2030 | |
| PHAB Standards and Measures |
The local public health agency (LPHA) CHAPS point of contact and project management team are responsible for planning and management of the entire CHAPS process. The structure and makeup of the team will depend on how you are conducting the CHAPS process: as a single entity, regional LPHA partnership, or partnering with other local organizations.
Roles can include
- Project manager: coordinates and manages the implementation of all CHAPS activities
- Agency decision-maker(s): public health director, division director, director of planning, etc.
- Health planner: gathers, interprets, and communicates data
- Facilitator: plans, facilitates, and records meetings
- Content experts: LPHA staff and community partners with knowledge across public health topics
- Administrative support: coordinates logistics and communicates with stakeholders.
- Partner organization(s): if the process is being co-led, hospital, agency, or community partner
- Community representatives
Gaps in skills can also inform who else in your community or region needs to be part of the process to inform best practices and quality engagement. OPHP staff can also help connect you to these resources and potential partners.
Determine if your internal team needs any additional training on
- CHAPS
- Project management
- Data collection (quantitative and qualitative)
- Public Health Accreditation
- Change management
- Health equity and community engagement
- Social determinants of health
- Strategic planning
- Facilitation
Why
The community health assessment and public health improvement plan are intended to be community-based processes and guiding documents that support the local public health agency, key stakeholders and community residents in addressing priority health issues. Once you have determined the internal roles of LPHA staff, create a group of key community or regional stakeholders. This group can:
- Advise the assessment process (data collection and community engagement).
- Engage community.
- Participate in prioritization of public health and environmental health issues.
- Develop the public health improvement plan.
- Form work groups to craft action plans to address priority issues.
- Be responsible for or advise implementation.
- Contribute to the monitoring and revision of action plans.
Who
The make-up of this group will be dependent upon your local process. For example, it can be an already formed group of local partners, such as a health care coalition, public health alliance, or LPHA staff representing different counties in a regional partnership. Or it can be a newly formed group for the purpose of guiding the CHAPS process.
Convening this type of advisory group is a great example of Public Health 3.0 and illustrates the chief health strategist role that public health plays. From this vantage point, it is also an opportunity for public health to strategically seek stakeholders beyond public health. The advisory group is one place to engage different sectors and community members. It is important to include sectors outside of public health as the Colorado public health system works to address and support priority issues such as climate change and behavioral health in ways that focus on the root causes of the issues and associated inequities. Engaging diverse perspectives in the data collection, prioritization, and decision-making activities will strengthen the validity, transparency, and potential impact of the assessment and planning process in your communities. Use a health equity framework, like the Bay Area Regional Health Inequities Initiative (BARHII) Framework as a guide for which sectors and parts of your community you can engage in this advisory group. See Phase: 2 Engage Stakeholders for further guidance on engaging stakeholders throughout the CHAPS process.
Advisory group engagement
This is group is composed of strategically selected stakeholders who meet regularly to advise the assessment process, participate in prioritization, then develop and implement the public health improvement plan.
The internal project management team should be a part of the advisory group, in addition to community organizations, civic leaders, elected officials, and consumers.
Recruit members who can influence systems, provide a voice to underserved communities and/or champion priorities. New members can be added at any time. This type of committee usually meets monthly, bimonthly, or quarterly, depending on the planned milestones and timelines.
The advisory group may range in size from a few people to 20 or more. If you have too many participants to reasonably manage, consider using topic-specific subcommittees, each with a representative to the larger steering committee.
A trained facilitator is useful to manage advisory group meetings, as this is where key decisions will be made.
- Contribute to the communication and promotion of the process and plan.
- Contribute to the evaluation of action plans and assessment and planning process to provide recommendations for improvements for the next cycle.
In addition to or in lieu of an advisory group, you may choose to do this work in partnership with another entity. Partnering with neighboring local public health agencies, community organizations within your jurisdiction, other government agencies, or hospitals can increase the efficiency and effectiveness of your CHAPS process. Colorado local public health partnerships have sprung up around conducting assessments on shared populations and implementing shared, county-wide and region-wide public health improvement plans. As LPHAs develop strategic partnerships to address pressing priority and emerging issues, variations of partnership models are needed to tackle issues that public health cannot tackle by itself.
If this is the route you take, consider developing a legal agreement such as a memorandum of understanding (MOU) to formally delineate roles, expectations, leadership, and funding.
A common time frame for the full CHAPS process is approximately 12 to 24 months. Use a timeline to outline how long you plan each phase to take. Use a work plan to outline more detailed activities, time frame, and person responsible for each phase.
Download a sample CHAPS Work Plan here.
Download the Colorado Assessment and Planning Requirements Checklist here. Click the "download" button in the top right corner for a fillable PDF version.
Talk with the OPHP Public Health Planner about
- Timing and work plan
- Requirements
- Partnerships
At any step in the process, connect with OPHP for guidance and support on
- Potential funding
- Data collection and sources
- Training and capacity building needs
Familiarize yourself and your partners with the:
Requirements for local public health agency community health assessments and public health improvement plans. Start with the Requirements for Local Public Health Improvement crosswalk. Pay close attention to the Public Health Act, which can be found at Section 25-1-501, CRS et seq. (Title 25 - Public Health and Environment - Article I: Administration - Part 5 Public Health Act - Subparts 1 through 3). This statute requires local and statewide public health improvement plans to be conducted every 5 years.
Phases and steps of CHAPS so you can formulate your local process, determine where your process may deviate, and note any questions for the Office of Public Health Practice, Planning, and Local Partnerships (OPHP). This discussion will help inform the overall CHAPS process with local examples.
State and national level standards for community health assessments and public health improvement plans, such as:
- Colorado Core Public Health Services/updated definition of Assessment and Planning capability.
- PHAB National Accreditation Standards and Measures
- Healthy People 2030 proposed framework and public health infrastructure objectives
- Public Health 3.0: A Call to Action to Create a 21st Century Public Health Infrastructure
Review existing assessments and plans to prevent duplication of effort, seek new stakeholders and partnerships, use data and priorities that have already been established, illuminate gaps, and help frame the scope of your process.
Here are recommended places to start:
- Your agency, last community health assessment and local public health improvement plan and process.
- Your agency, lessons learned from the last CHAPS process.
- Colorado's current and previous assessments and plans.
- Local needs assessments conducted by other governmental agencies, coalitions, or community organizations for relevant data and information that can be used throughout the process.
Who
Determine which organizational leaders in the community will need to be involved in this process ahead of time so they can support it. Then, determine how you will continually engage them in the process. Those with approving authority, such as agency leadership and your local board of health, will be some of the first levels of leadership you will work with.
These leaders may include:
- County administrator.
- County commissioners.
- Local board(s) of health.
- Public health/environmental health agency staff.
- Local hospital(s)
- Non-profit entities, including those outside of public health
- Other county governmental agencies, including those outside of public health
- School district(s)
- Service organizations
Consider additional key supporters. These are stakeholders who may or may not be formally involved in the process but who need to know about it early, so they can be supportive.
How
The community health assessment and public health improvement plans are valuable efforts to talk about health and environmental issues in new and different ways to impact the changes you seek. How the results of the assessment and the prioritized issues are communicated or framed can have a bearing on how they are interpreted, believed, acted upon, and supported. Phase 3 (Assess community), Phase 6 (Develop the plan), and Phase 7 (Implement the plan) all include recommendations to build a communications plan. Use those steps to take a closer look at communication methods and modes. Communicating the process and findings with leadership will be an initial test of your messaging, explanation, and context that you provide along with data results.
The resources needed to complete assessment and planning activities will depend on
- Size of the community(ies).
- Amount of in-kind resources (i.e. donated time, money, supplies, space, etc.)
- How extensive the assessment and planning process needs to be, based on what is already available.
Contractors
Some agencies may elect to consult or contract with other organizations that specialize in quantitative and qualitative research and/or assessment and planning for support with one or more of the CHAPS phases. OPHP maintains a list of organizations that local public health agencies have worked with over the years. You can reach out to ophp@state.co.us for questions and considerations related to contracting this type of work.
Operations
Develop a budget that includes the following:
Identify operational resource needs to carry out all phases of CHAPS. Note which are provided in-kind vs. those that need funding. Examples include:
- Meeting space
- Equipment (laptop, projector, conferencing capabilities)
- Supplies for meetings (flip charts, markers)
- Travel funding (mileage reimbursement to promote participation)
- Funding for producing a printable and/or online version of the community health assessment and public health improvement plan
- Funding for community engagement processes
- Staff training and capacity building if they are new to their role
Consider resource needs for monitoring and evaluating the impact of your plans. Contact state agencies, other LPHAs, or other community organizations who might be needed to provide data or technical assistance for the evaluation early in the process.
Determine if there are community partners who might also benefit from a public health improvement process and may be willing to contribute resources, such as
- Nonprofit hospitals: required to complete a community health assessment every 3 years.
- Community partners: may contribute staff time, supplies, equipment, meeting space.
- Public Health or Nursing Students: student project contributions.
Download a Sample CHAPS Budget Template.
Sample job descriptions:
- CHAPS Project Manager Position Description
- Health Planner Position Description
- CHAPS Facilitator Position Description
Personnel
Identify key positions and personnel needs in relationship to current staff resources and the scope of your process.
A single staff member may be used to fill more than one position and a consultant may also carry out the functions of a position (facilitation, data analysis, strategic planning).
Phase 2: Equity and community engagement
Use this phase to think through how you will engage a range of stakeholders throughout the CHAPS process to support equity and create a better assessment, plan, and implementation process. Local public health agencies are the required entity to carry out this process but it is intended to be done in partnership with the community.
Engaging stakeholders is important throughout all of the CHAPS phases. Since this can take months or years, be mindful of your engagement methods and adapt as necessary to respond to your community's needs and capacity for involvement. The community engagement strategies you use will be one way that you will be able to be transparent, build trust, and address equity through your assessment and planning process.
Community engagement is an essential function of public health and is found across national and state requirements as a public health best practice. Colorado Core Public Health Services and Capabilities model elevates Partnerships as a core service, including the act of engaging community member and cross-sectoral partners, agencies, and organizations. PHAB devotes Domain 4: "Engage with the public health system and the community in promoting health through collaborative processes" to this work as well and requires it in both the community health assessment and community health improvement plan processes.
Phase 2 tools &, templates
Shared Definitions
There are many reputable and wonderful community engagement and health equity resources that can guide your assessment and planning process. To maintain focus in CHAPS, we will reference a shortlist of recommended resources and encourage you to explore and adapt others to inform your local process.
Engaging a variety of different individuals, organizations, and sectors that have a "stake" in the process is a consistent activity throughout the CHAPS process. Regardless of the term used to define individuals that ultimately form the groups involved, it all falls within the definition of community engagement. Terms will be used interchangeably within guidance and local application and the same principles will apply.
Community engagement
As defined by the Colorado Office of Health Equity in the Authentic Community Engagement to Advance Equity resource, is:
- "a two-way exchange of information, ideas, and resources. Community engagement should offer opportunities to exercise power in decision-making. It should also consider the diversity of our communities - including culture and ethnicity - and seek to create an inclusive and accessible process."
PHAB guidance in Domain 4 expands on the definition to include:
- "Community engagement is an ongoing process of dialogue and discussion, collective decisions, and shared ownership. Public health improvement requires social change; social change takes place when the population affected by the problem is involved in the solution. Community engagement also has benefits of strengthening social engagement, building social capital, establishing trust, ensuring accountability, and building community resilience."
Equity
As defined by the Colorado Office of Health Equity, is:
- "when everyone, regardless of who they are or where they come from has the opportunity to thrive. This requires eliminating barriers like poverty and repairing injustices in systems such as education, health, criminal justice, and transportation." Colorado Office of Health Equity definition.
Equity and community engagement are then paired because you cannot do community engagement without addressing equity and you cannot address equity without doing community engagement. Conducting cyclical assessment, planning, and implementation processes can become a way to both educate and mobilize your communities. Seek out and build relationships with community champions and community organizers to inform community engagement efforts and data collection.
You and your partners are strongly encouraged to engage community members' lived experience along with traditional data sources to get the reasons for and solutions to equity-based health issues.
Furthermore, the Colorado Core Public Health Services and Capabilities operationalizes health equity and social determinants of health in the following capability definition:
- "The governmental public health system in Colorado will intentionally focus on improving systems and institutions that create or perpetuate socio-economic disadvantage, social exclusion, racism, historical injustice, or other forms of oppression so that all people and communities in Colorado can achieve the highest level of health possible. Governmental Public Health will have the requisite skills, competencies, and capacities to play an essential role in creating comprehensive strategies needed to address health inequities and social determinants of health."
To do this work, you need quality engagement practices delivered in culturally and linguistically appropriate ways to listen, learn, and act. These practices will then provide a foundation to collect data, make decisions, provide leadership, and ultimately inform how you will tell the health story of your communities, county, and region.
OPHP CHAPS tools and templates:
Additional and external tools and guidance:
By engaging in a variety of stakeholders throughout the CHAPS process in an intentional and thoughtful way, you can ensure that your assessment and plan reflects your community's voice and priorities. Without their involvement, you may miss aspects of their lived experience that shed light on potential root causes and local solutions that may not otherwise appear in your data collection processes or in the literature. With increasing efforts to address the root causes of your community's health issues in addition to addressing current conditions, their voice is ever more important.
Recommended resources
There are many resources on how to go about engaging stakeholders, conducting community engagement, and thoughtfully using the results of your engagement (new partnerships, data collection, etc.). Here are a few recommendations:
Use engagement to advance equity.
Use the Colorado Office of Health Equity's Authentic Community Engagement to Advance Equity tool. This tool includes recommendations for facilitating discussions on the importance of the assessment and plan in providing data, engaging the community, and prioritizing issues in ways that communicate health inequities.
True to the Public Health 3.0 "chief health strategist" role, this ongoing effort will result in partnerships building opportunities that may not have been imagined otherwise. Including a variety of perspectives and efforts are necessary to tell the lived health story of your community, county, or region. It is also essential to addressing health inequities and addressing them with meaningful, locally developed solutions.
Link with other community initiatives
With a focus on equity, engagement and a diverse set of stakeholders comes alignment with other health initiatives that are likely occurring within your community. The public health agency's role as leader and convener of this stakeholder process will promote local alignment of priorities, strategies, and resources to improve community-driven focus areas.
An initial meeting with these entities can determine whether they are collecting data that can inform your assessments and whether the issue and work they are championing can be supported through the public health improvement process. For example, the local hospital may be mandated to also conduct a community health assessment under the Affordable Care Act. Also, there may be community coalitions that are organized around a particular health issue, determinant of health(e.g., housing, transportation), or population (e.g., seniors/adolescents) that can contribute to or join your process.
Apply what you have learned
Use a community engagement spectrum or continuum to understand what types of engagement you are employing or would like to employ, why, and how. A cornerstone resource has been a public participation spectrum developed by the International Association for Public Participation. Through CHAPS peer-networking event, CHAPS Community Engagement Spectrum version was created to apply the recommendations in the spectrum.
Use best practices
The Health Impact Project developed the Health Equity Guide for government entities with a specific focus on "Share[ing] power with communities" as a way to use community engagement effectively. Best practices to keep in mind include:
- Remaining open to learning about community priorities
- Allowing time and space to get to know one another
- Identifying strategic opportunities for communities to contribute their expertise and knowledge
- Sharing resources to develop skills and capacity to partner with the health department
The CDC Practitioner's Guide to Advancing Health Equity is another resource that provides guidance on how to go about meaningful community engagement. As described in the Guide, it is important to understand the history of engagement in the communities you seek to support and work with. What has worked well or not in the past is important for your relationship building going into an engagement. Check out steps like these in the mini-version of the guide: Meaningful Community Engagement for Health and Equity. Tailor your engagement to be culturally and linguistically appropriate for the communities you are engaging with. Reference the National Standards for Culturally and Linguistically Appropriate Services (CLAS) in Health and Health Care blueprint.
Enter into community engagement with an open mind and respect that you may not know what you do not know. Because of this, it can be helpful to use an objective tool that facilitates the process of understanding what you and your partners know, what you need to learn, and where you can learn it from.
Here are two equity assessment tools that can get you started:
Community Engagement Assessment tool developed by the Nexus Community Partners organization is a self-assessment to ask why, how, and when you will engage. Racial Equity Toolkit developed by the Government Alliance on Race and Equity (GARE). See Step #3 for community engagement questions along with other GARE resources mentioned in the toolkit.
Questions to consider:
What training do staff need to meaningfully engage stakeholders? What resources do we have internally to engage stakeholders through community engagement activities and events? What resources do we have in the community that can help us manage and execute engagement efforts? (e.g., existing coalitions, other efforts engaging the community for different purposes, grants available, CSPH community health assessment class.) Reference the Colorado Office of Health Equity's Measuring Performance to Advance Equity for indicators that you can use to design a process and support your stakeholders so that you can achieve equitable outcomes.
The assessment tools will be useful again in the development of the community health assessment (Phase 3), capacity assessment (Phase 4), and public health improvement plan (Phase 5).
This type of engagement and with who will depend on the level and type of expertise you need to incorporate into the process. With your advisory group, identify the points at which it would be most helpful to engage stakeholders in your process and consider your community capacity for managing engagement efforts.
Stakeholders
Local customization of community engagement techniques is the key to making them work. While some of your stakeholders, such as advisory group members, will play a consistent role throughout your process, others may engage only at specific times. Also, consider any differences in power or communication skills among your stakeholders and explore ways to ensure that each participant has an equal voice in any given process. It is also very important that all stakeholders have a role that's purposeful, specific, and defined, and that their time and contributions are recognized and celebrated.
When to involve stakeholders depends on the role they will play and those associated activities. The scheduling of stakeholder activities will be driven by the timeline of your overall project and the related outputs and milestones.
Stakeholders whose support, approval, and/or funding that you need to make sure the process is successful from the start and able to move forward should be engaged first. In CHAPS, these are called "key supporters" and include the local board of health, LPHA staff, county commissioners, county administrator, and other community leaders. Stakeholders who will be involved in an ongoing advisory capacity, such as a steering committee.
- Before selection, you may want to take an initial look at community health data to aid in identifying steering committee members based on known health issues.
- Alternatively, you may already have a community group working broadly on health issues that can fulfill the role of the steering committee.
Coalitions or other organizations
Coalitions or other organizations working on a singular health issue should also be engaged as soon as the topic becomes relevant to the process.
- These groups can be managed as subcommittees with a designated representative to the larger steering committee to ensure alignment among all the groups.
Subject matter experts, Focus groups, and Stakeholder meetings
Interviews of subject matter experts and the facilitation of focus groups and stakeholder meetings are likely to occur later, during the assessment and planning phases. Engaging stakeholders through these mechanisms can:
- Elicit community perceptions of health issues
- Determine why certain health indicators look the way they do, including likely root causes
- Suggest strategies to address health issues, including programs or initiatives already planned or in progress
- Identify community entities in the best position to take the lead on an issue
You will know who you need to involve in this process, however, as public health works to address ever more complex health issues and the social determinants that influence health, consider this recommended list of potential stakeholders.
|
Who can... Impact the leading causes of disease, injury, disability, and death and/or the greatest health risk to our community? Represent populations that should be assured a voice in the process? Provide lived experience with the issue we are working to address? |
• Community-based organizations • Other non-health local governmental departments or agencies such as transportation, education, law enforcement, justice department, housing authority/agency, economic development, parks and recreation, planning and zoning • Human services • School board(s) • Environmental health organizations • Local hospital, other medical providers, health plans • Business community • Community members, especially those who will be impacted by the plan, such as youth, parents, seniors, LGBTQ, refugees and immigrants, and/or people with disabilities, etc. • Populations that are at higher health risk or have poorer health outcomes • Faith-based organizations • Civic groups such as Rotary Club or Lions Club • Media |
|
What other entities are also providing foundational public health services or addressing a pressing health issue? |
• Neighboring local public health agencies • Other non-health governmental departments or agencies • Community-based organizations • Local hospital and other medical providers • State or federal governments |
|
Who is in a leadership position to change or influence policy, impact large systems, provide a new service or contribute resources? |
• Elected officials • Local board(s) of health • Directors of community-based organizations • Public health director from a neighboring county • Community coalitions • Municipal leadership • Other non-health local governmental departments or agencies such as transportation, education, law enforcement, justice department, housing authority/agency, economic development, parks and recreation, planning and zoning • Area Health Education Centers (AHECs) • CEOs (or their designees) of local health-oriented businesses (e.g., hospital) • Community champions who may advocate and fundraise • Other agencies that would naturally take the lead on an issue that impacts public health (law enforcement, planning dept., school district, human services, etc.) |
|
What subject matter experts are need to inform the process? |
• Community members and trusted leaders in the community • Representatives and members of disparately affected populations • Community advocates/organizers that may provide a voice for hard-to-reach populations • Issue-specific experts at local, state and/or national level |
|
Whose support is needed to assure the process is successful? |
• Public health agency director • County administrator • Local board of health • Elected officials • Everyone engaged in your process |
Adapted from CHAPS 1.0 and PHAB reaccreditation requirements.
Engagement strategies
Stakeholders will be engaged throughout the process, so while they all do not need to be contacted immediately, it will be good to have a plan for who gets contacted when, in what manner, and by whom. Here are general recommendations:
Communications methods and techniques
LPHAs are more commonly including aspects of communities or partners engaged, how often, and in what ways in the action plans so that this effort is done in tandem with key activities to address the priority issue. Action plans are discussed in Phase 6.
Some stakeholders may "wear many hats" within the community and be involved in many volunteer and community efforts. Be mindful of this challenge and use it to inform how often they are engaged, in what methods or mode, and why. Hone your facilitation skills to be the most efficient with their time.
Build engagement and communication into your action plans
When engaging stakeholders for the first time, it will be particularly important to define expectations such as their role, time commitment, level of decision-making authority, how communication will occur, and intended outcome (e.g., a public health improvement plan). Many times, community members are overextended and may be reluctant or unable to participate in one more local effort. Providing them with a well-defined role, timeline, and a vision of the outcome communicates your resolve to get things done.
Minimize burnout
This approach can also help you negotiate the type of participation by specific stakeholders. For example, if an organization's leader cannot commit to regular meetings, ask her or him to delegate a representative and see if she or he would agree to serve as a subject matter expert. This will keep her or him engaged, even if she or he cannot participate in an ongoing manner.
Initial engagement
The health of a community is influenced by a number of factors, not all of which are under the public health agency's control. For some issues, other community entities may be in a better position to carry out strategies that improve public health. Learn more about addressing social determinants of health and how to create effective messaging from resources like the Colorado Office of Health Equity.
Face-to-face meetings
Your recruitment will be more successful if you determine the best method of making contact, instead of a one-size-fits-all approach. So, while some of the "usual suspects" may agree to participate after simply receiving a letter or email, you may get better results from other stakeholders, especially those who are new or deemed absolutely essential, through a face-to-face meeting.
Partners outside of public health
Potential stakeholders will need to understand the "why" behind your work in order to find shared beliefs and values that would motivate engagement. Learn more about messaging and communication, especially around complex issues such as housing and mental health at the FrameWorks Institute. The County Health Rankings and Roadmaps Action Center also provides concrete tools and resources to develop sound communication plans.
Determine if additional stakeholders would benefit the process. This may occur through mechanisms such as:
- Asking the steering committee who's missing
- Asking subject matter experts to recommend additional experts
- The emergence of new environmental and public health issues during the assessment phases.
- Realization of the need for further community input for prioritization and planning
New stakeholders may be added at any time. If new members are added to the advisory group, consider providing them with an orientation before their first meeting. Likewise, stakeholder positions may change individuals, such as county commissioners and leadership positions. Do your due diligence to get them up to speed so that you can maintain institutional knowledge in the process and incorporate the expertise and insights that a new individual will bring to the process.
Throughout the process, use a positive engagement strategy to acknowledge the contributions of all your partners and invite them to celebrate the achievement of milestones. A key part of the celebration is to acknowledge progress. When any milestone is reached, establish or maintain an ongoing communication mechanism to keep them informed and engaged to the degree that is appropriate for their role and level of interest.
The CDC cites common and instructive guiding principles of a community health assessment process. As you prepare for the process or reflect back on engagement, look at how many are tied to meaningful community engagement of diverse stakeholders.
Multi-sector collaborations that support shared ownership of all phases of community health improvement, including assessment, planning, investment, implementation, evaluation. Proactive, broad, and diverse community engagement to improve results.
- From Principles to Consider for the Implementation of a Community Health Needs Assessment Process (June 2013), Sara Rosenbaum, JD, The George Washington University School of Public Health and Health Services, Department of Health Policy.
- A definition of community that encompasses both a significant enough area to allow for population-wide interventions and measurable results, and includes a targeted focus to address disparities among subpopulations.
- Maximum transparency to improve community engagement and accountability
- Use of evidence-based interventions and encouragement of innovative practices with a thorough evaluation
- Evaluation to inform a continuous improvement process
- Use of the highest quality data pooled from and shared among, diverse public and private sources
Phase 3: Conduct a community health assessment
The steps of the new CHAPS Phase 3 guidance are meant to be followed chronologically and provide step-by-step instructions for conducting a Community Health Assessment (CHA). This guidance will help you tell the "story" of the health of your community. The results will inform prioritization and the local public health improvement plan, driving the work to address top health concerns over the next five years.
A community health assessment is a valuable public health role and responsibility. Enjoy piecing together data and telling your community's story!
OPHP CHAPS tools and templates:
- Colorado Health Indicators dashboard
- Colorado Health Indicators Dashboard Instructional Video
- Qualitative Data Collection Techniques
- CHA Checklist - fillable
Additional and external tools and guidance:
| Websites: |
| Public Health Accreditation Board |
| Core Public Health Services |
| Bay Area Regional Health Inequities Initiative Framework (BARHII) |
| Social Determinants of Health (SDOH) model |
| Colorado Health Information Dataset (CoHID) website |
| EnviroScreen |
Non-CDPHE Data Sources: |
| Community Tool Box |
Resources for thematic analysis: |
Data equity and visualization resources: |
The first step in a Community Health Assessment (CHA) is to select a model or framework to use during data gathering and analysis. The model is used to help think through the data, providing a defined approach to what data to gather and the storyline for describing the community’s health. Additional benefits of using a model include providing a structure of categories and naming conventions for organizing all the data, and to help identify topics where data aren’t available. It’s important to note that you do not need to use the same model for all activities like the presentation of the CHA results or in every phase of the Colorado Health Assessment and Planning System (CHAPS).
Why use a model for Community Health Assessment?
- Provides a defined approach to what data to gather and the storyline for describing the community’s health.
- Provides a structure of categorizing and naming conventions for organizing all the data.
- Identifies topics where data might not be available.
- Promotes health equity throughout the CHAPS process.
- You do not need to use the same model for all CHA activities like the presentation of results or even in other phases of CHAPS.
What are the considerations for selecting a model for Community Health Assessments?
- The public health law describes a comprehensive review of the data at the local level as a main activity of the assessment and plan.
- Ideally the model should emphasize a comprehensive equity perspective, looking at all aspects that influence the health of a community, and not only specific aspects like racial and other demographic diversity.
- The Public Health Accreditation Board (PHAB) requirements have heavy emphasis on the incorporation of health equity during the community health assessment process. Even if your agency is not currently seeking accreditation, following PHAB requirements is a good way to ensure that you are following national best practices.
- It’s beneficial to use a model that encompasses all of the Core Public Health Services so your CHA can clearly show how these services are available in your community as required by public health law.
What requirements drive the CHA data collection? Learn more about the history and requirements for community health assessments on the CHAPS Background and Requirements page. |
Do we have to use a specific model for the assessment?
- The CHAPS process does not prescribe a specific model that should be used.
- Selecting a model for the CHA that incorporates health equity is one of the most direct ways to ensure health equity is integral to the CHAPS process.
Is there a model that is most commonly used in Phase 3?
- The Bay Area Regional Health Inequities Initiative Framework (BARHII) is a model that is commonly used for community health assessments. The BARHII model does a great job of incorporating equity, including many social determinants of health, which helps to guide the collection of data resulting in a comprehensive review across a community. Additionally, the BARHII model includes all of the Core Public Health Services in the framework design.
- Colorado Health Indicators dashboard used the BARHII to help guide which indicators to include as a primary CHA tool supporting CHAPS work. The dashboard also organizes and visualizes the large set of metrics using the BARHII model.
- See below for examples of how local public health agencies have used the BARHII model to guide their assessment:
- Mesa County Public Health Department modified the BARHII model to meet their local assessment needs. See page 5 of the linked 2018-2020 Community Health Needs Assessment.
- Pitkin County Public Health used the BARHII model to guide data collection for their Community Health Assessment. They outlined their CHA findings according to each BARHII topic area. See the 2022 Community Health Assessment.
- Chaffee County Public Health used the BARHII model to guide data collection for their Community Health Assessment. While they reference the model throughout their assessment and plan, you can see the main areas of alignment at a glance in the “Key Findings” section starting on page 34 of the linked 2021 Community Health Assessment.
- See below for examples of other models used by local public health agencies for their assessment work:
- Pueblo County’s 2021 CHA process utilized the Healthy People 2030 Social Determinants of Health (SDOH) model. View Pueblo County’s 2021 Community Health Assessment.
- The MAPP 2.0 framework's Community Status Assessment, can help guide decision making related to data collection and analysis. It is a quantitative assessment for public health improvement planning and helps communities move upstream and identify inequities beyond health behaviors and outcomes, including their association with social determinants of health and systems of power, privilege, and oppression.
Much of the time and energy during this CHAPS phase is spent gathering and reviewing data for inclusion in the community health assessment. This section answers questions about where to find data and how to interpret it.
Access
Where should I start my search for data?
- The Colorado Health Indicators was created and designed specifically for CHAPS to assist with the community health assessment. Dashboard Instructional Video
- It is a comprehensive set of metrics that describe community health at the county, regional and state levels. The data are already pulled from over 30 different sources and it organizes the data so you can start reviewing right away.
- You are not required to use each data indicator from the CO Health Indicators. It’s mostly just a great place to start comprehensively looking at the data so you can better decide what next steps you need to take for this CHAPS phase.
- Using the Health Indicators also creates some alignment across counties and with the state by tracking some of the same measures
- The Colorado Health Information Dataset (CoHID) website provides access to state and local-level data and resources compiled by the Colorado Department of Public Health and Environment.
- CoHID Instructional Video
- Most of the dashboards available from CoHID have data available at the county level and here are a list of a few particularly helpful for CHA work:
- Chronic Disease
- Colorado Health Indicators
- Environmental Public Health Tracking
- EnviroScreen
- If you are unable to find the data you were looking for on CoHID or you’d like to see the data a different way (from how it’s been provided), you can submit a request using the Data Request System (DRS).
- There are other sources of data, besides those from CDPHE, that can be helpful in looking at data for the CHA. Below are a few particularly helpful places to look for data:
What should I do when there are small numbers in the data? What if my estimates are suppressed (not shown)?
- Sometimes estimates are suppressed due to small numbers geographically and/or demographically. When this happens, there are two suggested strategies for getting useful estimates:
- It’s perfectly acceptable to use aggregated years of data to get an estimate. Sometimes aggregated estimates are already available online and can also be requested from the data source. By combining multiple years of data, there is usually enough sample size to calculate a stable estimate at the county level. It is typical to combine 3 years of data for most sources. Due to the 5 year cycle of assessment and planning, it is not recommended to use more than 5 years combined for an estimate that will be used in a CHA.
- Often when the data are not available to the county level, they are available for the CO Health Statistics Region. While a regional estimate is not as specific as a county estimate, it still may be useful. If the regional estimate aligns with what is known to be true (from other data sources, anecdotal evidence, etc) in the community, then the regional estimate is still useful in telling the data story.
What is the best way to cite data sources in a CHA?
- The single most important thing is to cite the data accurately and specifically! Since the CHA informs several later phases in the CHAPS process and is repeated every 5 years, it is especially important to have proper information about the data used in the CHA. This will ensure that you can easily find the original data source again later if you need to reference it again. It will also provide greater transparency for others who want to utilize the data from your CHA to inform their own work.
- There is no prescribed format for CHA citation but make sure the following components are included in the chosen format:
- Primary data source (including the name of the dataset and the program/agencies who provide it);
- Data year(s);
- And website where the data were found (could be a primary or secondary source’s website).
- A primary data source is the name of the data collection system and the original program/agency who collected the data. A secondary data source may visualize and distribute that data, but are not the collectors nor original ‘authors’ of the data.
- Example using an indicator from the CO Health Indicators dashboard:
2021 Colorado Behavioral Risk Factor Surveillance System. Center for Health and Environmental Data Division, Colorado Department of Public Health & Environment. Accessed from: https://cohealthviz.dphe.state.co.us/t/HSEBPublic/views/CHITemplate-Redesign1_0-latest3-11m_16527278788750/CHI?%3Aembed=y&%3Aiid=2&%3AisGuestRedirectFromVizportal=y
- CoHID is a secondary data source, providing access to several data dashboards with data from numerous primary data sources. Make sure not to cite the name of the secondary source’s website where you found the estimate, but provide both the primary data source who created the data and also include the secondary source’s website address where you found the data.
What are the types of data used for CHAs?
- In the data world, there are two main types of data; quantitative and qualitative. Quantitative data are often more objective, counted or measured, and usually represented by numerical values (Height, age, distance, etc). Qualitative data are often more subjective, are descriptive and observational, and usually expressed using language (emotions, stories, quotes, etc). One type is not more valuable than the other; rather the two forms of data capture different dimensions of experience and complement one another. Check out this blog for more information about these two types of data.
What are the best ways to handle situations where there aren’t data to describe certain topic areas (aka ‘data gaps’)?
- Before deciding there is a data gap, it’s helpful to do a quick check of the approach while searching for that topic area. It’s easiest to keep an open mind about what data exist. It’s much harder to search for very specific information rather than to search by topic area.
- A useful mindset while searching for data sounds like “What data are available for tobacco use?” versus a less productive mindset of “Where can I find the exact number of people who smoked a pack of cigarettes per day in February 2022?”.
- Although the specific data that originally came to mind might not exist, there still may be data to describe this topic area for the community using what data are available.
- Utilize the partners and stakeholders in your network to identify data for the topics you are missing. Ask colleagues, community organizations, other local public health agencies, state health department staff, etc what data they use to describe the missing topic(s).
- Search for qualitative data that describes the missing data topic(s). [Read the Qualitative Data section for more information.]
- Data are not perfect so don’t expect the data story to be perfect. In other words, there won’t (and doesn’t need to) be an existing data measure for every detail of the data story. Use as much of the data and information that already exists to tell the story of the health of the community.
Should I collect my own data for the CHA?
- You are not required to collect your own data. In most cases, collecting new data from the community is not a necessary part of a CHA.
- Utilize as much of the quantitative and qualitative data that’s already been collected. It is not recommended to collect quantitative data because most has already been collected through traditional surveillance systems. If data needs to be collected for assessment and planning, it’s usually qualitative data around prioritization of community needs and interests. [Read the Qualitative Data section for more information.]
- Collecting new data is resource intensive, requiring lots of time, support, and money. And often the end result will not yield results that can be used for describing large populations in the community.
- Engage in conversations with the CHA project team, other health planners, and the OPHP staff to decide whether this is the only option for collecting certain data of interest. The OPHP staff have access to data people who specialize in designing data collection tools and can also make connections to academic partners who can assist with this activity.
Analysis
When is it best to use rates, proportions and frequencies?
- Rates are really helpful for comparing over time and comparing with other geographies (county, region, state, etc) because the rate has accounted for changes and differences in population sizes. Typically infectious diseases, mortality data, and injuries are described using rates. Age-adjusted rates are useful because these calculations have accounted for the differences in populations by age in a community as well as the differences in diseases by age.
- Ex: The suicide death rate for County A is 16.3 deaths per 10,000 people.
- Proportions, often reported as percentages, are helpful for describing the magnitude of the burden. Typically morbidity data including chronic conditions and diseases are expressed as proportions.
- Ex: 6.5% of Colorado adults have diabetes.
- Frequencies, also known as counts or numbers, should be used as little as possible in CHAs. The biggest concern around using frequencies has to do with confidentiality and privacy of individuals in the community. Additionally, analyzing frequencies over time is tricky because changes to populations or circumstances make it harder to understand any observed differences. The best time to use a frequency is to quantify things or places but not people.
- Ex: There are 5 community clinics in County A that currently accept Medicaid.
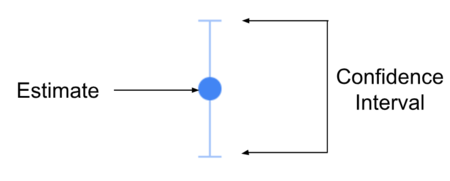
What is a confidence interval and how does it determine statistical significance?
- Simply explained, a confidence interval is a way to describe the certainty of an estimate. For a 95% confidence interval, if we measured a sample 100 times, 95 of those results would fall within the specified range of the confidence interval. In other words, 95% of the time the “true value” is between the lower and upper limits of the confidence interval range.
- Watch this video for a helpful explanation of error and confidence intervals.
- One of the simplest and fastest ways to determine statistical significance between two estimates is to compare the confidence intervals. See illustrations below:
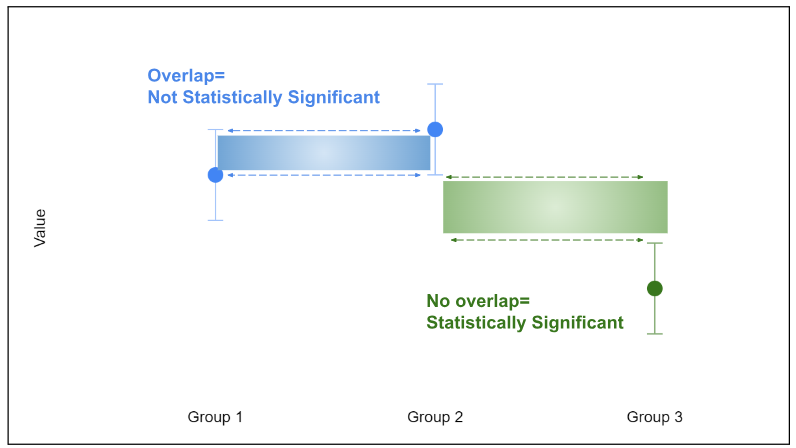
- The ‘true estimate’ can be anywhere within the range of the interval. So when confidence intervals overlap, that means there is a chance that those estimates could be the same value. And that means the estimates are not statistically significantly different. For example, there is no statistically significant difference between Groups 1 and 2.
- When the confidence intervals do not overlap, this means there isn’t a chance that the estimates are the same. Therefore the estimates are statistically significantly different. For example, the difference between Group 2 and Group 3 is statistically significant.
- The wider the range of the confidence interval, the less certain we are of the estimate. In other words, there are more possible values that the ‘true estimate’ might be.
- The more narrow the range of the interval, the more certain we are of the estimate. In other words, there are fewer possible values that the ‘true estimate’ might be.
Why is statistical significance important in CHA work?
- The large volume of data included in a CHA makes it complicated to understand where the greatest areas of strength and need are without a tool to help narrow it down. Using confidence intervals to help understand where the community is statistically significantly different is a useful tool for narrowing down to the most important themes from the data.
Qualitative data is non-numeric data that describes characteristics or qualities. It provides an opportunity to dig deeper into the context around the quantitative data that you have collected. This can help to tell a more nuanced story about why you might be seeing certain trends in your community’s data. This section answers questions about when and why qualitative data is used as well as how to approach collecting and analyzing qualitative data.
Why do I need qualitative data if I have lots of quantitative data?
- There is a lot of the data story that is not told by the quantitative data. Often qualitative data helps provide context and frames much of the story that can’t be told by quantitative data alone.
- Qualitative research provides the opportunity to engage your community, explore people’s perceptions, experiences, opinions, and beliefs, giving us a deeper understanding of the issues. It also helps to capture the unique language, culture, and views of a particular population.
- Qualitative data can help you generate ideas for upstream issues to focus on in your public health improvement plan.
Can I use qualitative data to supplement the missing quantitative data?
- Yes, using qualitative data is a great way to fill in where there are gaps in the topic areas covered by quantitative data. But make sure to include relevant qualitative data wherever it fits into the CHA and not only just where quantitative data don’t exist.
- Remember that you will likely not have a huge sample size for qualitative data collection due to the time and resources that qualitative methods can take. Therefore, be cautious about making generalizations about the entire community based on your qualitative data. However, it is still a great source of information!
How do I collect qualitative data?
- Listed below are some of the most common qualitative methods. Each method has their unique pros and cons. For example, one-on-one interviews give the interviewer opportunities to ask follow up questions so that respondents can provide more detail and explain themselves as needed. However, they also take more time to carry out and require additional staff time to schedule, record, and transcribe. Take some time to think through each method before determining what will be best for your agency’s capacity and goals:
- Open-ended survey questions
- One-on-one interviews
- Focus groups
- Town halls
- Photovoice projects
- View OPHP’s Qualitative Data Collection Techniques resource to learn more about these strategies
- The Community Tool Box is a great resource for learning more about when and how to use different methods of qualitative data collection.
What considerations should I keep in mind when designing qualitative data gathering methods?
- Involve community members when developing questions to ensure they’re culturally appropriate & understandable.
- Avoid public health jargon & keep wording simple.
- Avoid leading questions, 2-part questions, & questions based on assumptions.
- Pilot test the questions with a small group for feedback.
- Consider approaches in other languages if your community has a large non-English speaking population.
- Shorter surveys/interviews can help increase response rates.
- Train interviewers to remain neutral and consistent to avoid influencing responses.
Analysis
What is thematic analysis?
- Thematic analysis is one of the most common ways to analyze qualitative data. It involves reading through the data (for example, a transcript from an interview or written responses to long-answer survey questions) and identifying patterns or “themes” in the different responses. It is a flexible and accessible approach to qualitative data analysis and does not require any fancy tools or software, although there is software available if you choose.
How do I use a thematic analysis approach to analyze my qualitative data?
- First, get familiar with your data. Read through all responses to any surveys. Transcribing, or writing down, interview and focus group dialogue is also a key part of analysis and can help you familiarize yourself with the data.
- It is helpful to record interviews, focus groups, or other dialogue that you will be using as a source of qualitative data. Make sure to get permission from participants prior to recording.
- Assign initial codes to all lines of the text or transcript. Codes are labels that you assign to different pieces of the text to identify important topics and concepts. See the example below:
- Generally, there are two methods for determining codes:
- Inductive coding: This is when you come up with codes to reflect the data as the text is reviewed and categorized for the first time. These codes can be refined as the process moves along.
- Deductive coding: Before reviewing the data, you come up with predefined codes based on existing data or literature. These are then applied to the text as you review the qualitative data.
- It is a best practice to have two people work on coding the same data. They should work separately and then once they have coded a few responses, they can come together and make sure that the codes match. If there are any differences in codes between the two coders, those should be discussed before deciding on final codes to use.
- Look at the list of codes that you have generated and how frequently they come up across the various surveys or interviews. Search for common themes and group your codes by theme. Review these themes & think about how they relate to different health indicators.
- Resources for a more in-depth overview and additional examples of thematic analysis:
- How to do thematic analysis (Blog post)
- Qualitative Data Analysis for Health Services Research: Developing Taxonomy, Themes, and Theory (Journal article)
- An overview of qualitative research methodology for public health researchers (Journal Article)
- TIP: All LPHA staff have access to peer reviewed articles through the Public Health Digital Library. Learn more about how to access the library here.
How do I know the number of people I should interview or survey?
- An important concept in qualitative research is “thematic saturation.” Saturation refers to a point in your research when you begin to notice the same themes coming up again and again. Eventually, as you are interviewing or reviewing responses, you will likely notice that you aren’t seeing any more new themes. This is usually an indicator that you have received responses from enough people to draw some conclusions about the question that you’ve asked or the population that you are researching.
One of the best practices in community health assessment is to narrate the story of health across the community. In other words, use quantitative and qualitative data to tell the story of what's happening in the community.
Why is data storytelling useful in community health assessments?
- Extremely large amounts of data are gathered during the community health assessment process and can easily lead to an overwhelming amount of information that will need to be communicated to multiple audiences with varying levels of data knowledge.
- Data Storytelling makes data and statistics more approachable for yourself and your audiences.
How do I tell a data story?
- Social Math is one approach to simplifying complex statistics by reframing them in a more familiar context. Here is a LINK to an article describing what and how to use Social Math.
What’s the difference between data analysis/interpretation and data storytelling?
- Data analysis and interpretation happens during the data gathering process where you understand what each indicator means and is saying about the community.
- Data storytelling is a strategy to communicate the findings or results of all the data that were analyzed for the community health assessment.
Does data storytelling work for all audiences?
- In general, data storytelling will effectively communicate the important messages to most audiences. Sometimes it will make sense to provide different levels of statistical information about the data to different audiences.
- For example, it might be appropriate to share the statistically significant differences with the Executive Director of your LPHA so they can see how data decisions were determined. Whereas it would not be beneficial to share the statistical significance of data to community members.
What are some examples of data storytelling?
Data visualization is a huge piece of the CHA phase because it is one of the primary ways of communicating the story of health for the community. This section provides information on what is needed for CHA submission and tips for current best practices in data visualization. Resources to explore more on data visualization practices are listed at the end of this section.
Is there a required format for the CHA?
- There is no required format for the final product of the CHA data and information.
What is required for the CHA submission?
- The CHA must be approved by your local board of health and then it may be sent to OPHP. LPHAs must also submit proof of board approval, such as a copy of an email exchange with the board of health or a copy of meeting minutes.
- LPHAs may submit their CHA on its own, upon completion OR agencies may wait and submit their CHA & PHIP together.
- Both CHAs & PHIPs should be turned in via a Google form upload. The form can be accessed here: https://forms.gle/VtiHD3fRrjK3xvuw9. If there are any questions about this form, please reach out to ophp@state.co.us
What are some of the ways to visualize the CHA data and information?
- Many assume that they need to provide their CHA in a traditional report format, but that is often not the most useful way to share the information. Other format options include a slide set, data dashboard, series of one-pagers covering each section/topic area,
- The previous statewide health assessment provides examples of both one-pagers and a data dashboard.
Is there a best way to visualize the CHA data and information?
- The best way to visualize the CHA results is to do it in the most useful way possible. Design the product(s) to be meaningful for the audiences you will be sharing the information with and in a format that you can easily use.
- A traditional report is not a format that is easily presented to audiences, so slides may work better and can be easily modified for a variety of presentations and audiences.
- A data dashboard might easily display the data, but can be resource intensive and require a lot of maintenance over time. How many people will use it, how often, and if the data are already visualized on other data dashboards are all important considerations for whether a data dashboard will be meaningful and useful for your CHA data and information.
- Discuss with your colleagues, partners, OPHP staff, and other LPHA health planners to hear how they are packaging their CHAs and why they used those formats.
How can I use the CHA products for other work?
- If you intentionally design your CHA information in a useful way, it will help be relevant for several other future activities:
- The CHA data will be used for later CHAPS phases for the Capacity Assessment and Improvement Plan. The CHA data can be informative for demonstrating strengths or advocating needs related to the Core Public Health Services.
- The stronger the CHA product, the smoother the CHA process will go in future CHAPS cycles.
- The data and information created from the CHA can be used where other data are needed in your public health work like grant writing and program evaluation.
What are some tips for incorporating health equity into the visualizations of the CHA data?
- Remember that population based data are data about people. So treat the data as people and not simply as points of information.
- Some data can be used to simply describe. Not all data are suitable for comparisons. Consider the appropriateness of comparing groups of people.
- An easy practice to use when handling data about people is to avoid making comparisons across groups of people; rather make comparisons within groups of people.
- Example of the less ideal comparison across groups of people:
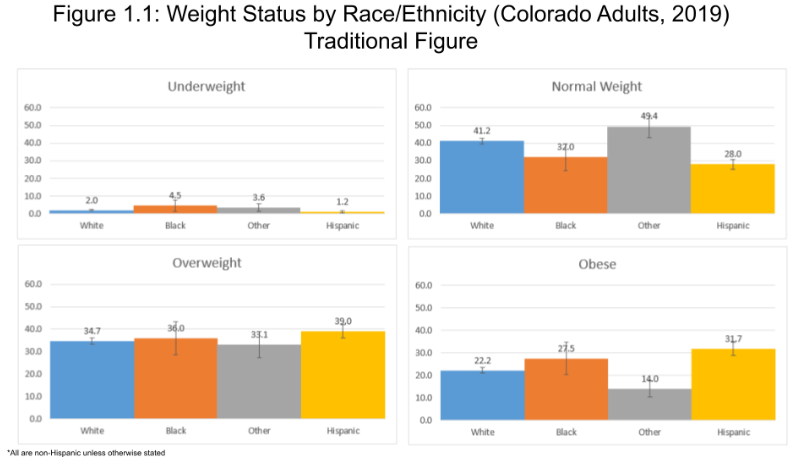
- Example interpretive statement for Figure 1.1: Hispanic adults are more obese (31.7%) compared to White (22.2%), Black (27.5%), and Other (14.0%) adults.
- This is an inappropriate comparison because it creates the standard that the racial/ethnic populations should have the rates of other groups of racial/ethnic populations; when the standard should be to decrease the proportion of obese adults and/or increase the proportion of adults with ‘normal’ weight.
- Example interpretive statement for Figure 1.1: Hispanic adults are more obese (31.7%) compared to White (22.2%), Black (27.5%), and Other (14.0%) adults.
- Example of more ideal comparison within groups of people:
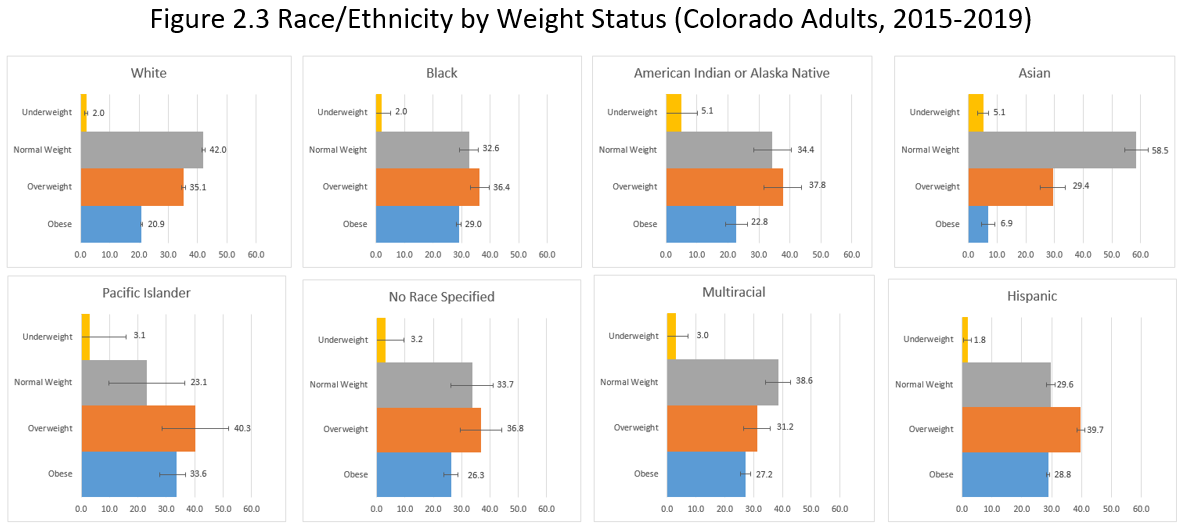
- Example interpretive Statement for Figure 2.3: Asian adults have the highest proportions of people with normal weight (54.5%) compared to Asian adults who are overweight (29.4%) or obese (6.9%).
- This is an appropriate way of describing the population and doesn’t compare them or set a precedent of what the proportions should be based on race/ethnicity.
- Example interpretive Statement for Figure 2.3: Asian adults have the highest proportions of people with normal weight (54.5%) compared to Asian adults who are overweight (29.4%) or obese (6.9%).
- Consider using different types of figures to help engage the audience and avoid unintentional comparisons.
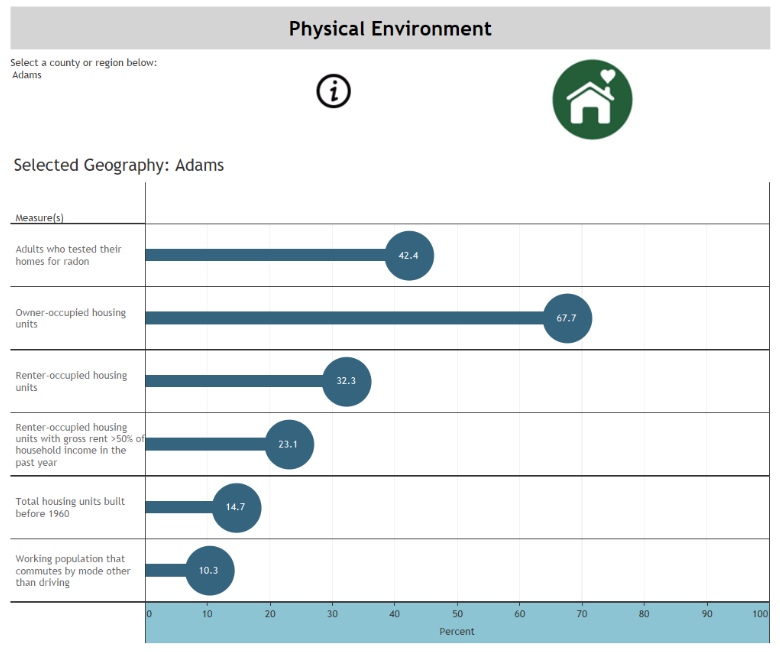
- In the example below, several different data points are displayed on the same screen. If traditional bars were used to display them, it would unintentionally lead audiences to compare them like they were part of a stacked bar graph displaying data for a comparison. So in this example from the CO Health Indicators dashboard, ‘lollipop’ graphs were used to distinguish the data points and to be interpreted individually.
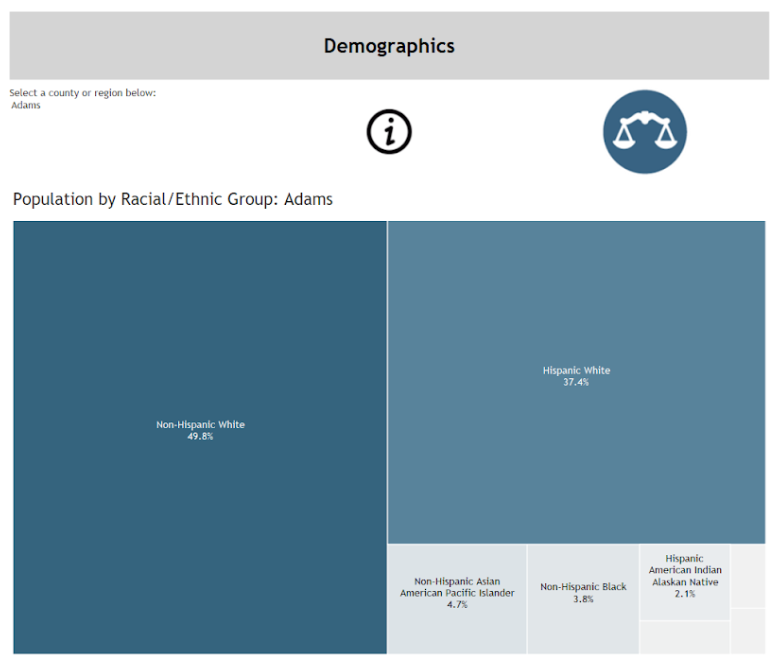
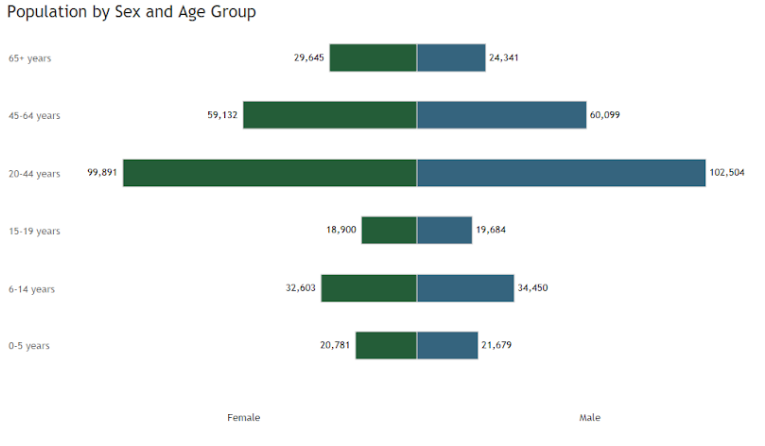
- The next example, also from the CO Health Indicators dashboard, provides examples of visual options for displaying demographic characteristics. It’s not useful to compare the percent of people by demographics within a community because there are no defined demographic percentages that a community should have (i.e. We don’t, nor should, have definitions like ‘communities should have at least 25% Hispanic population’ or ‘30% of a community should be less than 18 years of age’). The ‘tree map’ and ‘butterfly’ graph do a better job describing and visualizing what the demographics are for the community than a traditional table or bar graph.
- Often quantitative data are presented alone as tables and figures and aren’t the full story of what is happening in the community. Provide context alongside the quantitative data to explain the whole ‘story’. This can be done in a number of ways that are described in the Data Storytelling and Qualitative Data sections of this chapter.
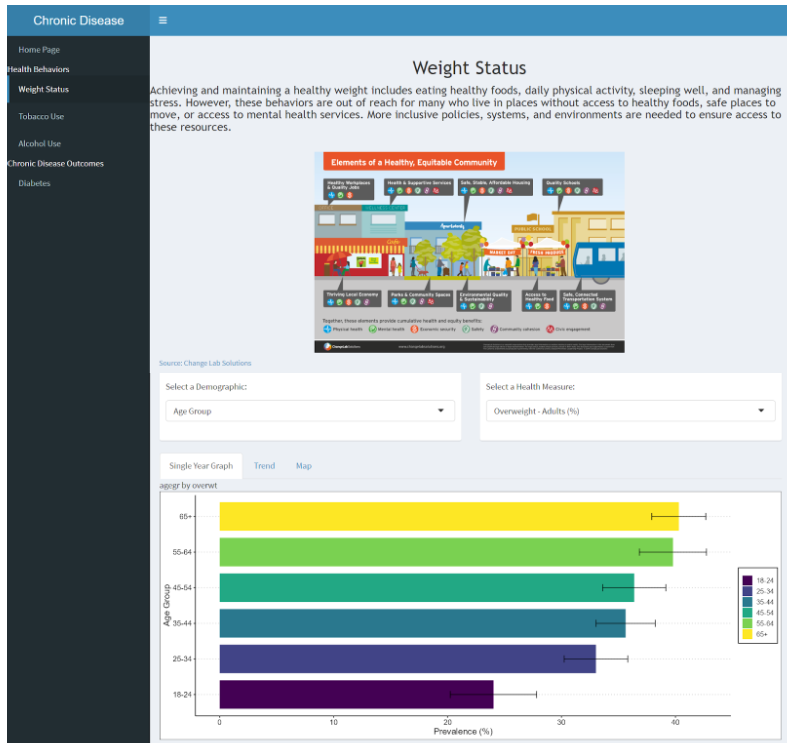
- The example below comes from the VISION dashboard and provides an example of what it looks like to include context alongside the quantitative data.
- Focus on the protective factors versus the risk factors wherever possible.
- For example, instead of only including in the CHA the measure for obesity in the community, include the measure for the percent of the population that has a normal weight.
- This doesn’t always make sense, particularly where a community has significant differences for the negative health outcome. Often in this scenario, it makes sense to describe the negative health outcome and then also present a positive health outcome alongside it.
- Example: If a county has a statistically significantly high percent of people who are obese, include both the estimates for obesity and normal weight along with a narrative about increasing the population of people with normal weights.
- Data equity and visualization resources:
Click here to download a fillable PDF version of CHA Checklist (with space for taking notes):
The checklist for completing your Community Health Assessment includes the following components:
- Select model for data organization
- Using the selected model as an outline, review and pull data from CO Health Indicators for my county
- Review and pull data from other dashboards on CoHID
- Explore other sources of quantitative data
- Explore and include potential sources of qualitative data
- If need is determined, collect local data
- Analyze and interpret the gathered data to decide which data to include in assessment
- Design data product(s) to visualize selected data
- Incorporate a narrative voice to tell the data story of health in the community
- Incorporate best visualization practices to clearly and equitably tell the data story
Phase 4: Assess capacity
Use this phase to assess capacity to achieve community health goals. The capacity assessment is a process for measuring the ability of an LPHA and its partners to deliver or ensure public and environmental health services, programs, and activities.
Make note that you will use the results of your capacity assessment from Phase 4 throughout the prioritization process in Phase 5. It is important to consider how Phase 4 and 5 are related and how one influences the other before choosing and designing a capacity assessment.
The Colorado Public Health Act requires every local health plan to "assess capacity and performance of the county or district public health system" and "Identify financial resources available to meet identified public health needs and to meet requirements for the provision of core public health services." (Section 25-1-205 Subpart 2b).
However, the act does not require a specific process, content, or reporting format; therefore, each community will decide the best method for collecting, sharing, and using this information based on local needs. Some tools that can be used are linked in Step 3.
OPHP CHAPS tools and templates:
- CHAPS Capacity Assessment Guide
- SWOT Analysis Template
- Core Public Health Services Capacity Assessment Matrix
- Qualitative Data Collection Techniques
Additional and external tools and guidance:
| PDFs: | Websites: |
| Building Skills for a More Strategic Public Health Workforce: A Call to Action | County Health Rankings and Roadmaps |
| Public Health Accreditation Board (PHAB) |
Begin the phase by determining the area of capacity to assess and to what extent you will determine capacity. Choose the area that will best support the overall assessment and planning process. This will look different for each agency and depend on various factors, including:
- Findings from the community health assessment conducted in CHAPS Phase 3
- Current delivery of foundational public and environmental health services and capabilities within the jurisdiction
- Whether incorporating quality improvement methods and/or sustainability planning into the process is an identified agency goal
- Whether the agency is preparing to seek national public health accreditation and/or is interested in measuring performance against state and nationally recognized public health performance standards
View the CHAPS Capacity Assessment Guide here.
Understanding the capacity of both your agency and your community can influence the priorities, goals, and strategies of the public health improvement plan. It can also help to assure successful implementation of your plan. Capacity assessments are especially helpful as agencies move towards highlighting and addressing root causes of health inequities in their communities.
Below are three examples of capacity areas to consider. The first example is required to gather enough information to prioritize issue areas coming out of your CHA. However, you can choose to assess additional areas to better understand both internal and external capacity to deliver foundational public health services to serve your communities. If additional capacity issues arise, know they can also be considered in the Phase 5 prioritization process.
| Capacity area | When to assess benefits | Partners involved | Examples of questions to consider |
| Capacity to address prioritized public health issues. This type of assessment examines the ability of your agency and partner(s) to address public health issues in your community(ies), county, or region. | Assess as part of the community health assessment (Phase 3), as a parallel phase, or as part of the prioritization process (Phase 5) Provides rich information about the ability, potential capacity, and feasibility of the agency and local partners to come together to address priority issues. | • Agency leadership and governing authority, such as local board of health • CHAPS oversight committee • Community stakeholders (ranging from community members and representatives to organizations and community leaders) | • Type of support an organization can provide • Interest level in addressing priority issues with partners • Equity-specific questions regarding populations served and impacted • Workforce expertise to address priority issues |
Colorado Core Public Health Services and Capabilities. It is the responsibility of each local public health agency to regularly assess its ability to provide or assure Core Public Health Services and Capabilities. A core services capacity assessment examines the range to which these services are fulfilled. Services and capabilities were identified and drafted by Colorado's public health community and established into rule by the Colorado State Board of Health in 2011 and amended in 2019. | Assess as part of the community health assessment (Phase 3) or as a parallel phase, or an ongoing agency process. Results will determine an agency's capacity to deliver core public health services and meet the requirements of the Colorado Public Health Act. Colorado Core Public Health Services and Capabilities provide a clear guide for the delivery of quality public health services. It will be important for agencies to know how their agency aligns in order to address any gaps that may present barriers to the overall delivery of quality services. Health equity and social determinants of health is a foundational capability. This assessment area also provides an opportunity to understand an agency\'s capacity to address root causes of health inequities, educate staff, and address social issues that influence and determine health. | • Internal agency staff • External partners and customers can provide input • Agency leadership and governing authority, such as local board of health | • Likert-scale questions regarding alignment with service and capability operational definition |
Agency or system performance. Besides looking at programming, staffing, and resources to meet core services and/or priority areas, you may also elect to assess agency performance. PHAB standards require agencies to address quality improvement and performance management | Assess as part of the community health assessment (Phase 3), as a parallel phase, or an ongoing agency process. Performance management and quality improvement are ways to understand how an agency or system is functioning, which is a useful input to the development of an agency strategic plan. | • Internal agency staff • Customers | • Customer satisfaction • Professional and workforce development • Progress made on program, policies or process goals • Infrastructure capacity |
Based on the scope of assessing capacity, here are some recommended resources to review for your process:
- Previous agency capacity assessments. Some local public health agencies have a history of assessing the public and environmental health needs in their community in relation to existing services and required resources.
- Each Colorado local public health agency completes and submits a self-assessment to the Office of Public Health Practice, Planning, and Local Partnerships (OPHP) via the annual survey. This survey is meant to document the degree to which the agency provides or ensures core public health services. For information on your agency's responses and for support in interpreting the data, contact OPHP.
- In 2019, all local public health agencies will have completed a public health and environmental health core service cost assessment. Your individual county results as well as results from your region may provide insights into strengths and weaknesses in agency capacity.
- Workforce development. Insufficient staff and expertise are cited barriers in Colorado's public health system. Identify whether data on staffing, resources, and activities have been collected recently for other purposes. This may include documents such as annual reports, grant activities/deliverables, and applications prepared by your agency or partners. For the national context, de Beaumont Public Health Workforce Interests and Needs Survey (PH WINS) provides insights into the public health workforce that may be beneficial to compare to your local context. Gaps and assets may reveal valuable information that have bearing on your agency's capacity to provide quality public health services or implement a public health improvement plan. Check out the Building Skills for a More Strategic Public Health Workforce: A Call to Action, also led by the de Beaumont Foundation, for ways to act on results from the capacity assessment.
- Capacity assessments conducted by other organizations providing public health or environmental health services for your jurisdiction, if available. Discuss with partners to learn more and to gain additional local perspectives.
Collect new data if your agency and partner(s) need to know more. Use a method or approach deemed most important to the community health assessment and planning process. Aim to gain a wide variety of perspectives of the agency/system's ability to address priority issues and/or provide public health services. Reference Phase 2 when considering the best way to engage stakeholders in collecting data.
Consider these data collection techniques:
- Community asset inventory (may already be part of the community health assessment process)
- Strengths, Weaknesses, Opportunities, and Threats (SWOT) analysis
- Core services baseline review analysis or core service cost assessment result analysis
- Facilitated input discussions with stakeholders
- Key informant interviews
- Online partner survey
See CHAPS Qualitative data collection techniques for more guidance.
Other templates that may be helpful include:
Once data collection is complete, analyze and interpret the story it tells. Highlight areas of strength and strategic opportunities for moving toward increased capacity in whichever capacity area(s) you have chosen. These strategic capacity-building opportunities and assets may ultimately become key goals or strategies in your public health improvement plan over the next five years or the agency's next strategic plan.
Now that you have analyzed capacity data, it is time to summarize and share the information based on how the results will be used. Here are a few examples of how the results can be used.
|
Capacity area |
Use of results |
|
Capacity to address prioritized public health issues |
• Phase 5 - Prioritization process: Results can help make decisions about the potential priority areas identified in the CHA to drive the public health improvement plan (PHIP). • Phase 6 - PHIP: Results can inform action steps to address important capacity shortfalls, including the implementation of capacity-building and performance-improvement activities and ongoing evaluation of capacity-building progress over time. • Collective impact: Results can provide opportunity(ies) with system partners who are identified to take the lead on individual components of the larger plan (PHIP). • Results may provide insight into root causes of health inequities and influence action plans in the public health transportation plan. |
|
Colorado Core Public Health Services and Capabilities |
• Phase 5 - Prioritization process: Results can help make decisions about the potential priority areas identified in the CHA to drive the public health improvement plan. • Phase 6 - PHIP: Results can inform action steps to address important capacity shortfalls, including the implementation of capacity-building and performance-improvement activities and ongoing evaluation of capacity-building over time. • Determine an agency's capacity to meet the requirements of the Colorado Public Health Act and align with Core Public Health Services and Capabilities • Agency annual report, strategic plan, performance management plan and/or quality improvement plans. • Determine health equity/social determinants of health capacity gaps and strengths. • Communicate and advocate for public health and environmental health services to a variety of different audiences (e.g. county commissioners, funders, local partners). • Support PHAB accreditation process. |
|
Agency or system performance |
• Phase 5 - Prioritization process: Results can help make decisions about the potential priority areas identified in the CHA to drive the public health improvement plan. • Phase 6 - PHIP: Results can inform action steps to address important capacity shortfalls, including the implementation of capacity-building and performance-improvement activities and ongoing evaluation of capacity-building over time. • Agency annual report, strategic plan, performance management plan and/or quality improvement plans. • Support PHAB accreditation process. |
Phase 5: Prioritize issues
Use this phase to prioritize issues that arose during the assessment to determine a few focus areas for the five-year public/community/regional health improvement plan. A well-defined priority-setting process will help you and your stakeholders determine how to strategically direct resources toward issues where they will have the greatest impact. These are recommended steps and can be done in the order that makes the most sense for your local planning and action needs.
Make note that you will use the results of your capacity assessment from Phase 4 throughout the prioritization process in Phase 5. It is important to consider how Phase 4 and 5 are related and how one influences the other before choosing and designing a prioritization process.
Prioritizing issues is a cross-cutting public health activity required in the Colorado Public Health Act, updated Core Public Health Services and Capabilities, and the Public Health Accreditation Board accreditation process (PHAB).
Phase 5 Tools & Templates
OPHP CHAPS tools and templates:
Additional and external tools and guidance:
| PDFs: | Websites: |
| NACCHO Guide to Prioritization Techniques | The Community Guide (CDC) |
| Public Health Digital Library |
Aim to identify 5-10 potential priority areas to consider.
Review the results of the community health assessment and the list of main topic areas to consider for prioritization that were included in the assessment. Also, review the results of any capacity assessments completed in Phase 4 for potential topic areas to consider for prioritization. Focus areas may include public health issues, environmental health issues, capacity/infrastructure needs, or issues that address the social determinants of health or health equity.
Selecting focus areas for public health improvement helps ensure that limited resources can be targeted and important issues can be spotlighted. Focus areas are high-priority, high-visibility issues that organizations serving the community will come together to champion. Efforts to support the focus areas will occur alongside the maintenance of regular public health activities.
Select a prioritization method and determine how, by who, and when you will execute the process. The design of your prioritization process should take into account your capacity assessment needs and the amount of additional information you will need to gather on potential priority areas. This may happen at the same time, before, or after you complete your capacity assessment, depending on your unique needs.
Choose a prioritization method
A prioritization method is used to determine a few local public health improvement focus areas by further examining and ranking important issues that have been identified through the community health assessment and capacity assessment processes. When determining a method, ensure that you outline a structured process that you will follow that incorporates guided discussion among all participants.
Recommended resources include:
- CHAPS Prioritization Matrix is a commonly used method in Colorado
- Guide to Prioritization from the National Association of County and City Health Officials (NACCHO) provides guidance on a variety of different methods
- Focus on What's Important from the County Health Rankings and Roadmaps Action Center provides further guidance on the methods and process
Choose criteria
The following criteria should be used to discuss, evaluate, and score each potential priority area:
- Significance to the community's health
- Existence of associated strategies that can be implemented successfully and are likely to have a sustainable impact
- Presence of community support, leadership, and capacity to move the issue forward
- Impact on health equity
Questions to consider for the facilitated discussion are detailed in Step 4.
Determine who to involve
The prioritization process is an important way to gain buy-in from those in the best position to influence outcomes of the public health improvement plan and ensure that under-represented communities and participants have a voice. Being strategic in your selection of participants means you have identified a role for everyone involved in the process, for example:
- Advisory group
- Decision-makers who can impact policy adoption, implementation or enforcement
- Potential funders that may contribute toward addressing an issue (e.g., a municipality or hospital)
- Community organizations or neighboring local public health agencies (LPHAs) that may offer to enhance or provide a new program
- Community advocates that can give voice to the underserved
- Potential champions who can generate support, advocate and fundraise
- Public health agency staff who may be responsible for implementation
- Other government directors who would naturally take the lead on an issue (law enforcement, planning department, transportation, school district, human services, etc.)
Be sure to clearly communicate the participants' roles and level of decision-making authority to the group ahead of time. Determine and be transparent about the level of control that participants have in the prioritization meeting. Is it the role of the participants in the meeting to make the final decision on priorities or to make recommendations to the Board of Health or other entity? Note that the public health agency need not be the lead organization on every community health priority. The more engaged stakeholders are in terms of being able to make decisions, the more likely that advocates and lead organizations will step forward.
There are probably many groups already focusing locally on priority health issues. Some may be addressing an issue with great success while others may be struggling because they lack funding, staff, or other resources, or they may be using an ineffective strategy. A prioritization process can help stakeholders align by focusing energy, funding, and other resources on the same areas and respective strategies that result from this process.
Facilitation
Determine who will facilitate the meeting or meetings. The prioritization process will involve a considerable amount of discussion, both before issues are scored and ranked and afterward, to validate or change the rankings and to determine the number of priorities given levels of capacity. If you feel like you do not have the capacity to provide skilled, neutral facilitation of the prioritization process within your agency or community, contact OPHP. OPHP can assist with identifying a facilitator who can help guide the group toward consensus and moving forward.
Documentation
Documenting the process, method(s), who is involved, how the prioritization process was created demonstrates the integrity of your process. It is a PHAB requirement as well as a best practice in being transparent about a critical part of the CHAPS process.
Design a process
Combine previous decisions about the method, who to involve, and how to create your prioritization process. This will provide direction for a facilitated discussion with key stakeholders to systematically determine which issues should have a more targeted and planned focus over the next five years. The five-year goals are to "move the needle" on the issue, by either improving capacity or positively impacting a health outcome in a measurable way.
Gather additional information with the goal of creating a more complete profile of each potential priority issue for the purpose of decision making. For each potential priority issue be sure to provide information about each of the following criteria areas.
| Criteria | Description | Examples of where to find information |
| Significance to the community's health. | • The prevalence of individuals affected or at risk (e.g., mortality, morbidity, and injury rates). • The degree of health disparities or impact to subpopulations. | • Phase 3 Community health assessment • Reference primary data sources in Phase 3 • Phase 4 Capacity assessment • Engage a subject matter expert |
| Existence of associated strategies that can be implemented successfully and are likely to have a sustainable impact. | • Existence of strategies/best practices likely to have an impact. • Level of community readiness and support for change (including political will). | • Public Health Digital Library (Free access for Colorado LPHAs) • County Health Rankings Roadmap - What Works for Health • CDC Guide to Community Prevention Services • CDPHE Communities That Care communities and facilitators • Engage a subject matter expert |
| Presence of community support, leadership, and capacity to move the issue forward. | • Local organizations that are prepared to take the lead. • Sufficient resources, including staffing and funding, are available or obtainable. | • Phase 4 Capacity assessment • Engage a subject matter and community expert(s) and representative(s) |
| Impact on health equity. | • Incorporates a broader understanding of the priority issue inequities and disparities. • Are there population-based, primary prevention policies that improve physical, environmental, social, and economic conditions that affect the issue? | • Phase 3 Community health assessment |
Presentation format
Determine the best format(s) to present this information to stakeholders participating in the prioritization process to ensure they have a common understanding of the issues and all of the information needed to select priorities. Methods of delivery include:
- PowerPoint presentation
- One-page issue summary profiles
- Infographics
- Gallery of posters
- Report
Depending on your group, provide adequate information either before the prioritization process or during to ensure everyone has had an adequate amount of time to take in the information and to be prepared to make a decision.
Convene your stakeholders and facilitate the prioritization process you have designed. A thorough prioritization process will probably take three to four hours or longer, depending on the number of stakeholders and the number of issues. It may be structured as one or more meetings.
Sample agenda: (Could take place over one to three meetings)
- Purpose of the meeting/background
- Set meeting norms (also known as ground rules)
- Overview of decision-making roles and process
- Criteria for scoring/ranking
- Presentation of issue profiles with facilitated discussion
- Scoring/ranking of each issue
- Facilitated discussion on rankings
- Select final priorities
- Identify the next phase and steps in the planning process
The initial part of the meeting should provide background in terms of purpose, the role of the group, the decision-making process, and method of scoring. Consider setting ground rules or meeting norms as well. Choosing priorities can be challenging, as decisions will be difficult and not everyone's preferred issue will be selected. Ask the group to brainstorm norms for working together (e.g., confidentiality, respecting one another's opinions, etc.) and record them on a flip chart that all participants can see during the meeting. Ask participants if they can agree to all the norms. When a norm is broken, the facilitator can remind the group by referencing the flip chart.
The next part of the meeting will be the presentation of the issue. These are the five to ten issues up for consideration to be focus areas for the public health improvement plan. The objective of this activity is to educate the participants about the issues, provide enough background so they can score them, and have a discussion so that participants can exchange thoughts and ask questions. This part of the meeting will take the longest, you may want to allow a half-hour to present and discuss each issue.
Following the presentation and discussion of the issues comes the prioritization method that you have designed. Depending on the size of the group that you are working with and the method that you have chosen, this may occur in-person or through the use of technology.
The final part of the meeting is selecting priorities based on the discussion of the rankings. Scoring and ranking are not perfect processes. As such, the group should discuss how the rankings come out. The facilitator can use questions such as the following to prompt discussion:
- Is there a natural cutoff point for the highest-ranking issue?
- Do these issues seem like they are ranked in the correct order?
- Are there any criteria (like a political will or lack of a lead agency) that may make a particular issue difficult to implement regardless of its score?
- Of the highest-ranked issues, are there any that you think are not doable, and if so, why?
- Of the lowest-ranked issues, are there any that you think are doable that should be considered?
- Of the top issues, how many should be public health improvement priorities?
- Who is identified as the lead agency for the top issues, and how does this affect the overall number of priorities that can be selected?
At this point in the process, the group should be close to consensus on all or most of the issues. A show of thumbs or use of the clicker can indicate consensus or disagreement. If there is disagreement among several members, either a discussion should continue or the group may decide they need more information before coming to a consensus or compromise. As decisions are made on focus are priorities, record them. Reflect any notes having to do with voting, dissenting opinion, or any further actions needed before a consensus or compromise can occur.
End your meeting by discussing the next steps of the process. The priorities will need to be developed into action plans by workgroups (explained in Phase 6 - Develop the plan). Consider what communication might need to occur with stakeholders who were not able to attend. Help the participants understand and/or determine their potential roles in future steps. Lastly, celebrate the completion of this pivotal milestone in the public health improvement process.
Phase 6: Develop a plan
Use this phase to develop a five-year local community health improvement plan (CHIP) based on the results of assessment activities and the selected priority focus areas. The PHIP will become the road map for community and regional partners to make improvements to the public health system and ultimately the population's health. It will illustrate your county or regional public health needs, describe priorities for health improvement, include partners to be involved, document the steps to get there, and provide a method for evaluating progress.
There are a variety of proven processes to create a meaningful process and plan. These are recommended steps and can be arranged to best fit your local needs.
Phase 6 tools and templates. Click to download:
- CHAPS Action Plan template - Option 1
- CHAPS Action Pan template - Option 2
- CHAPS Logic Model template
- Sample PHIP Outline & Best Practice Examples
Important elements of a public health improvement plan
By now, your public health agency and advisory group have led a community-based process to examine health and environmental data and service capacity. You have also selected top focus areas or priorities for improvement. Together, these components tell the health story of your communities. The next step is to act on what you have learned by developing priority action plans for implementation and evaluation.
Shared definition
Creating a public health improvement plan has become a standard practice within the public health field. It is recommended by the National Association of City and County Health Officials, mandated by the 2008 Colorado Public Health Act for all local public health agencies, and required for voluntary accreditation by the national Public Health Accreditation Board (PHAB), which defines a plan as:
- "... a long-term, systematic effort to address public health problems on the basis of the results of community health assessment activities and the community health improvement process. A plan is typically updated every three to five years. This plan is used by health and other governmental education and human service agencies, in collaboration with community partners, to set priorities and coordinate and target resources. A community health improvement plan is critical for developing policies and defining actions to target efforts that promote health. It should define the vision for the health of the community through a collaborative process and should address the gamut of strengths, weaknesses, challenges, and opportunities that exist in the community to improve the health status of that community."
- -Public Health Accreditation Board Acronyms and Glossary of Terms Version 1.5, December 2013 (Adapted from: United States Department of Health and Human Services, Healthy People 2010. Washington, DC)
To the extent that this plan can impact your communities, always keep in mind that it is more than just a public health agency plan (research strategic plans for more information on how to do that). PHAB further defines a plan to be community-driven:
- "While the health department is responsible for protecting and promoting the health of the population, it cannot be effective acting unilaterally. The health department must partner with other agencies and organizations to plan and share responsibility for health improvement and advancing equity. Other sectors and stakeholders have access to additional data and bring different perspectives that will enhance planning. The health improvement process is a vehicle for developing partnerships and for understanding roles and responsibilities."
-Public Health Accreditation Board Standards and Measures Version 2022, Domain 5, Measure 5.2.1 A: "Engage partners and members of the community in a community health improvement process".
In summary, the PHIP serves as a measurable, outcomes-focused plan for your community to:
- Inform, engage and mobilize your community(ies)
- Align policy and community efforts
- Investigate and address social determinants of health and health inequities
- Outline shared action plans for your public health agency and community partners (e.g., hospitals, schools, transportation, environmental groups)
- Support grant applications with data and information
- Inform and engage with the state public health improvement plan to strengthen partnerships and maximize efforts
The plan is not limited to these benefits. Find the best ways to leverage this process in your community to use assets, engage your community and meet their unique needs.
Public Health Act requirements and timeline
Requirements
The Colorado Public Health Act of 2008 (Section 25-1-501, CRS et. seq.) requires a public health improvement plan to include the following six components:
- examine data about health status and risk factors in the local community
- assess the capacity and performance of the county or district public health system
- identify goals and strategies for improving the health of the local community
- describe how representatives of the local community develop and implement the local plan
- address how county or district public health agencies coordinate with the state department and others within the public health system to accomplish goals and priorities identified in the comprehensive, statewide public health improvement plan
- identify financial resources available to meet identified public health needs and to meet requirements for the provision of core public health services
- not be inconsistent with the statewide public health improvement plan
CHAPS provides guidance on meeting these requirements along with an emphasis on health equity and community engagement. Steps are in alignment with Public Health Accreditation Board (PHAB) Standards and Measures and are continually updated to reflect best practice. Agencies seeking accreditation should visit the PHAB website to review the latest guidance and documentation requirements. Reviewing the full set of PHAB standards and measures will provide useful information throughout the development and implementation of your public health improvement plan.
Timeline
Local and state public health agencies are required to carry out this process on a five-year cycle.
It's recommended that local assessments, prioritization, and, if possible, completed plans be submitted prior to each statewide plan to inform the development and implementation of the state plan. The next state health assessment is due in 2024 and the next state plan is due in 2025.
We recognize that not all Local Public Health Agencies are on the same timeline, so if you have any questions about when your next plan is due, reach out to us at ophp@state.co.us.
OPHP CHAPS tools and templates:
- Evidence Based Strategies Websites for Action Planning
- CHAPS Logic Model Template
- CHAPS Action Plan Template - Option 1
- CHAPS Action Plan Template - Option 2
- Sample PHIP Outline with Local Examples
- Local Board of Health Approval Guide & Fillable Form
Additional and external tools and guidance:
A well-thought-out process will ensure that the plan's development and execution is successful.
Scope
The scope of the plan will depend upon factors such as the end goal(s), regional public health and community partners involved, capacity, and whether or not your agency is using the plan to apply for accreditation or re-accreditation. Discuss and define the "right scope" of the plan with your advisory committee so that it is usable by all involved, measurable, meets requirements, and has the potential for impact.
You will also want to discuss the potential uses of the plan. It may be used to advocate for funding, to support grant applications, or to engage other sectors and define public health in a county or region. The scope and potential uses of the plan will help inform the following steps, guide implementation, engagement, communication, and evaluation.
This conversation will also be a valuable time for those involved to connect work done in the assessment phases with future ability to act on priority issues. The plan needs to be a solid connection between the two.
Planning process
Determine meeting schedule and logistics, such as location, frequency, length, agendas, communication method, etc. to complete the planning process. The number of meetings will depend on the size of your community and stakeholder group, and the number of priorities chosen.
Check on communication methods between those involved to ensure all are providing and receiving materials in a timely manner to review and take action. Also, check that everyone is doing an expected amount of work based on their original commitment to the process. Revise and update the process if need be. It is likely many involved will be volunteering their time. Take the time to thank them.
Prepare to delegate components of the plan and the following recommended steps to those involved. Allot adequate time for communication, discussion, and inclusion of stakeholders to participate. Determining strategies for an action plan or designing an evaluation plan will require specific skill sets and/or knowledge to accomplish. Consider these needs early on so that you have the capacity to engage additional subject matter or process experts. This may lengthen the process time but the engagement is worth it.
Engage advisory group
Re-engage your advisory group for the second part of this community process. An advisory group, a best practice for this work, can help foster the momentum of implementing the plan after it is developed by acting as a resource when barriers arise, as well as assisting in monitoring and evaluating progress. Provide adequate communication to the group about the assessment results, uses, and dissemination, as well as requirements and future needs of the plan to keep your decision-makers up to date. New stakeholders can be added at any time but now in particular is when additional stakeholders with different types of needed expertise within the priority areas can be included in the process. Be prepared to provide information based on their familiarity with the process thus far.
Determine needed resources
Just as you determined resources for the assessment, determine the resources needed to develop and implement the public health improvement plan.
Useful questions to consider:
- What is the timeline of our process?
- Are there any deadlines driving it and if so, what can be accomplished in the allotted time frame?
- Is your oversight group prepared to help provide guidance, input, and investment of time and resources?
- How will you engage your oversight committee group who will help guide the plan? (Think meeting location, structure and access as well as what they will commit to helping with.)
- What other partners do you need to engage to help fill information gaps or gain additional community perspectives?
- Will you need to engage subject matter experts to inform strategy development for priority areas?
- Do you have evaluation skills on staff or within the advisory committee?
- Will you use a consultant or partner with the Colorado School of Public Health?
- Will a variety of sectors be involved in the creation and implementation of the action plans?
- Do you or your stakeholders have grant writing experience to apply for grants to implement priority area action plans?
Ultimately, you need to ensure that you, your oversight committee, and partners have the knowledge, skills, partnerships, and resources on hand to develop and implement a public health assessment to the best of your abilities.
This step will depend on your local process. Discuss with your internal team and advisory council to determine your needs and capacity for engaging more stakeholders. Engagement is discussed in more detail in Phase 2, however, the following points are recommendations to keep in mind.
Involve different sectors
- When discussing the root causes and potential capacity for addressing your priority health issue(s), identify the different stakeholders that are already involved and working in this/these area(s). If an issue includes transportation barriers, engage transportation entities. If an issue overlaps with human services, engage both governmental and non-profit organizations. If an issue includes the built environment, engage those who are responsible for land use and planning. Engaging groups who may not be the typical players as early as possible (preferably in the assessment phase) so that you can collaborate moving forward to reduce duplicative efforts or fill gaps in services. Having sound subject matter expertise can also provide insight into aiming for policy-level solutions that have a broad base of support.
Address health inequities and social determinants of health
- Including diverse stakeholders, subject matter experts, and community voices throughout your process will help you understand the context of the issues and inequities that you seek to address. This will unearth the root, systems-level causes contributing to an issue. By having the "right people at the table" especially in the workgroups, you will all be more prepared to incorporate the strategies that address social, cultural, economic, and educational causes of priority health issues.
Assessment and plan accessibility
- Develop final products that are accessible and trackable by your partners. This will ensure transparency in your process and make it easier for your advisory group and any additional stakeholders to contribute to monitoring and evaluating the plan. This requirement is also reflected in PHAB Version 2022 Standards and Measures for Initial Accreditation Measure 5.2.3, "Implement, monitor, and revise as needed, the strategies in the community health improvement plan in collaboration with partners."
Communication
- Develop effective communication that resonates with your communities. If you have engaged a broader set of stakeholders and have involved them in different parts of your process, you can craft and test these messages together. Challenge your stakeholders to identify jargon or terms that may be misunderstood, diluting the effectiveness of your communication, and come up with locally defined ways to communicate.
Begin developing the plan by gathering available resources and insights. This work will be done by a core group of stakeholders, which may include all of the advisory or steering committee or a mix of committee and agency staff members.
Useful questions to consider:
- What are the requirements for a local public health improvement plan (PHIP)?
- What are the priorities identified in your last PHIP?
- Have you reached out to current and potential partners to learn about their priorities in your community, county or region?
- Are there specific efforts to address health inequities happening in your community, county or region?
- What are other current local and/or regional priorities?
- What are the current state public health and environmental health priorities?
- How does this information inform your plan process?
Collect and review requirements and additional relevant materials. The following are recommendations and only a start to your process. Continue by inquiring with agency staff and stakeholders who have been involved in the process before for their insights into the process and what has worked well in the past and currently.
|
|
Document |
Purpose |
|
Requirements |
Community health assessment and public health improvement plan requirements for local public health agencies, public health directors and local boards of health. Use to guide entire process as well as determine capacity. |
|
|
|
Outlines responsible party, process requirements, approvals, timeline and link between local and state processes. |
|
|
|
Colorado Core Public Health Capability: Assessment and Planning Note: Most applicable resources will be linked when available. |
Required assessment and planning knowledge and skill capacity. |
|
Relevant materials |
Past improvement plans developed by your agency |
Note significant findings and investigate changes or trends. Review actions plans and communication plan. |
|
|
Health improvement or action plans conducted by other entities in your community, county, or region |
Supplement your plan. Prevent duplication of effort. Determine gaps in who is addressing community needs/priorities. |
|
|
Public health improvement plans from other jurisdictions |
Awareness of how similar counties/local public health agencies have carried out their planning process. |
|
|
Colorado public health improvement plans: |
Align priorities, goals, strategies, and partners where and when appropriate. Opportunity for engagement and relationship building between local and state entities around shared priority issues. |
Delegate components of the public health improvement plan to focus specifically on priority areas. This will depend on the number of people involved and the expertise they bring to the process.
Who should be involved
- Breaking this process down into workgroups will provide an opportunity to bring in additional content experts or individuals who can represent subject matter expertise which also includes the lived experience of those who will be impacted by the plan. This may include those who have not been participants thus far. They may also have a stronger working knowledge of what it will take to implement strategies, make an impact in your communities as well as have evaluation, funding, and implementation capacity. Consider capacity gaps and seek stakeholders who can bring process expertise, such as evaluation. Look into the priority areas to see if any new stakeholders have been identified thus far.
- If you have not already, consider involving community advocates or organizers that can give a voice to underrepresented populations or those who can help address relevant health disparities. They can help engage communities that otherwise might not participate in public health activities, and may help tailor your strategies to appropriately fit the population. See Phase 2: Engage stakeholders for more ideas.
Responsibility
- The priority area workgroup(s) will be responsible for collecting any additional data and research necessary to make decisions about goals and strategies. They will use this information to develop an action plan (Step 5). They may also contribute to an evaluation plan, providing local knowledge about how to communicate and promote the action plans. Finally, they may potentially serve as partners in implementation (Phase 7). The meeting logistics and frequency will have been determined in the initial planning process (Step 1) of this phase.
Use this step to design action plans, logic model, and to identify strategies. The main part of the public health improvement plan will be the priority area action plan(s). An action plan is where priority area workgroups document how the agency and partners are going to address the priority issue, when, how, by how much, and by whom.
Action plans are multi-purpose tools that will be used to guide implementation, support accountability, and enable you and your partners to review and revise the plan. Thave can also serve as a communication tool and aid in monitoring and evaluation. Throughout this phase, look for ways that you can adapt these recommendations to support your planning process and to develop efficient and effective plans that are feasible to implement.
To that end, review this entire step to inform what additional information and activities are needed for priority area workgroups to complete.
Required components
Review the requirements in Domain 5 of the PHAB Standards and Measures for both Initial Accreditation and Reaccredition. It is important to consider both as the initial accreditation guidance covers best practices and requirements for a community health assessment and improvement plan, reaccreditation requirements highlight additional areas for growth.
CHAPS action plan
CHAPS guidance builds on these requirements through the development of an action plan. See the CHAPS Action Plan template (Template 1 | Template 2) for guidance on including the following components:
- Priority area with a description of the issue that includes relevant indicators and contributing factors/root causes of the issue
- Goal
- Strategy (read below for more in-depth guidance on strategy identification)
- SMART objectives
- Indicator(s) for monitoring and evaluation
- Reach/target population/community engagement
- Evidence-based, locally actionable strategies
- Major activities or action steps
- Timeline
- Entity or entities responsible for implementing
- Date completed/Status
Include additional fields as necessary to support the viability of the action plan and to clearly communicate how you will address the priority issue. There are many different types of guidance around action planning. This is an important process, so build plans that work well for you and your partners. County Health Rankings and Roadmaps also offers helpful guidance on the action planning process and product(s) along with curated tools and resources. Remember, there are a variety of ways to do this work, choose processes that will use the data you have collected to make decisions and lead to action.
Logic model
If you would like to take your planning process further to connect and communicate higher-level goals, consider using the CHAPS Logic Model template (click to download). You can find guidance on how to link your action plans and logic model in the OPHP CHAPS Action Planning presentation from Public Health in the Rockies. County Health Rankings and Roadmaps Action Center also recommends a Tearless logic model resource for additional insight into the process.
A logic model will also be a valuable activity and product to use to communicate progress and evaluate impact (Step 6 of Phase 6 and Phase 7).
Strategy identification
Take an adequate amount of time to research, identify and discuss strategies. Keep the overall plan goal, scope, and capacity in mind, while also looking for creative, innovative solutions that address the root causes of public health and environmental health issues.
Within the workgroup meetings, begin with understanding the factors contributing to the priority issue and information learned during the prioritization process, such as evidence-based strategies, locally informed strategies and solutions, partners, and existing efforts.
Depending on your process, you can choose a formal identification method such as a prioritization matrix or decide through group discussion. Here are criteria to discuss in selecting strategies:
- Likelihood of population impact
- Capacity to implement
- Impact on health disparities and inequities
- Community assets and resources
- Ability to measure change
- Ability to evaluate for process improvement and/or impact
- Political/community support
- Policy level strategies exist
This is the time to address upstream, social influencers of health. Invest time and resources into identifying equity-specific strategies for the plan. For example, seek out and identify upstream policy level strategies that have the potential to influence societal and cultural norms around priority health issue areas.
Refer back to the equity and engagement assessment tools recommended in Phase 2. Act on the results of these assessments by incorporating equity-based strategies. Ask important questions such as the following set included in the 2019 State Assessment and Planning process from the Office of Health Equity:
- Could the efforts burden traditionally underserved communities?
- How will this proposed strategy benefit traditionally underserved communities?
- Will affected communities have decision-making power in the decision-making process?
- How are affected communities involved in defining success?
- Are there mechanisms in place for affected communities to hold decision-makers accountable?
The following recommended resources will help you dig deeper:
- Public Health Digital Library
- National Association of County and City Health Official (NACCHO): Compendium of NACCHO Policy Recommendations 2017
- CDC A Practitioner's Guide for Advancing Health Equity: Community Strategies for Preventing Chronic Disease provides community-level strategy examples.
- Health Equity Guide: A project by Human Impact Partners provides support for how local health departments can be more strategic about address equity issues.
View the document below for a list of additional national resources for identifying evidence-based strategies:
Here are additional resources developed by CDPHE programs for evidence-based strategy identification:
- CDPHE Communities That Care communities and facilitators - Seek out local CTC facilitators for opportunities to partner in shared priority areas and risk and protective factor-related strategies.
- CDPHE Oral Health Resources for Public Health Improvement Plans - Check out this resource specially curated for LPHAs to identify and incorporate oral health data, resources, partnerships, and strategies into your PHIP. It is a unique health issue with strategies that can have cross-cutting impacts.
To further illustrate how chosen strategies are addressing root causes, social determinants, and influences on population health and environmental health, consider using a tool such as the NACCHO Community Health Improvement Matrix. It overlaps a strategy identification process with the socio-ecological model to visualize different levels of strategy intervention. By visualizing "where" all of the strategies are being implemented in a population, you can see if you are choosing a comprehensive set of strategies. Importantly, strive to include policy and culture influencing strategies for greater impact on population health and for addressing root social causes. Strategy identification is an iterative process. After using this guide, go back to revise strategies, if necessary.
Check out other Colorado public health improvement plans to learn more about local strategies chosen across the state. Agencies and partnerships choose a wide variety of strategies to meet their local needs and are influenced by their local context.
Report final action plans back to the advisory group for final discussion and inclusion in the plan.
Create a process to keep your action plans accountable, current, and responsive to internal and external factors. Use this process to monitor action plans on an ongoing basis to improve and revise them as progress is made and changes occur.
A process should include how changes will be tracked, when and how often, who will be responsible, and when and how revisions will be made. Ultimately, this activity will begin to answer the question, "Did we do what we said we were going to do?" and contribute to the evaluability of the overall plan. PHAB Initial Accreditation Measure 5.2.3 states:
"Effective community health improvement plans should not be stagnant, but dynamic to reflect the evolving needs of the population served. Health departments should continuously work with multi-sector partnerships to evaluate and improve the community health improvement plan."
To keep your plans "dynamic" consider the following questions:
When developing a process
- Has a data tracking system been identified to generate information on indicators?
- Will a monitoring system be used, such as software, databases, Web-based dashboards, and/or community-balanced scorecards?
- What indicators do you look at and how often?
- Are there adequate resources to complete data collection and analysis?
- Will the monitoring plan answer useful evaluation questions that can inform process or strategy improvement?
- How will stakeholders access action plan status?
- Do you have the information that you need in your action plan template?
If a monitoring system is chosen...
- Who will populate the system?
- How often is data updated and from what sources?
- What are the potential negative impacts? How will these be mitigated?
- What is the initial development cost, if any? Who might want to share the costs? What is the cost to update and maintain? At what frequency? Financial sustainability?
If revisions need to be made...
- What are the criteria for action plan revision?
- Will it be based on quantitative or qualitative data sources?
- Will it be influenced by state or national scale changes (e.g., CDPHE state health improvement plan, Healthy People 2030)
- What is the time frame?
- Who will need to approve?
- What will you change?
- Objectives: Actual aim, or just the number you were trying to reach?
- Strategies: If what you are doing is not working, how will you change it?
- Indicators: Will you change the indicator if you realize that it is not measuring your objective or the indicator is not suitable?
This step will provide the base set of information needed to evaluate action plans and the assessment and planning process.
Why?
CHAPS is a cyclical public health improvement planning process that provides the opportunity for an agency and your partners to increase impact and improve the process over time. By monitoring the action plans, all involved will have a sense of progress or change due to the process. When you wrap up one cycle and prepare for the next, however, plan to evaluate the overall process to include both outcomes of the action plans and the assessment and planning process in general.
What can you evaluate?
Amongst the advisory group, determine what you would like to evaluate in 2-3 years' time. Consider these specific areas to include:
- goals and objectives determined in the action plan(s)
- process or outcome measures/indicators identified in the action plan(s)
- implementation of strategies (intended and unintended outcomes)
- community engagement throughout the process from data collection through implementation (satisfaction, inclusivity, quality, reach, etc.)
- partnership engagement throughout the process (satisfaction, inclusivity, geography, sectors, quality, reach, etc.)
- public health improvement planning process
- capacity to address health inequities
- communication methods and reach
This can be a general outline and at this point is most helpful in informing the information you collect so that you have it available to evaluate. Keep in mind that you do not need to evaluate everything. Choose the most meaningful activities, inputs, outputs, and products of your process and invest in collecting the data you need to monitor and evaluate them. Circle back to your action plans to make sure you are optimizing that process to collect information that can be evaluated.
Evaluation design and resources
At the time you intend to evaluate, determine the optimal type of evaluation, such as a process or outcome evaluation. At the minimum, your evaluation should help you answer the following questions within each area you have chosen to evaluate:
- Did we achieve the goals we set out to?
- What were the impacts of the plan?
- Was there an equity impact?
- What do stakeholders want to know?
- What went well?
- What were the challenges?
- What improvements should we make and how?
Seek out specific evaluation resources, engage your partners that have evaluation expertise and community impacted by the plan to guide your process. Here are some recommended resources to take a deeper dive into this specific process:
- Evaluate actions - County Health Rankings and Roadmaps Action Center
- Measuring Success: Evaluating Comprehensive Community Initiatives - Community Toolbox
- Program Evaluation for Public Health Programs: A Self-Study Guide - CDC
- Designing Program Evaluation To Advance Equity - CO Office of Health Equity
"Evaluation allows you to be sure the strategies you are implementing are working in the way you intended and that your efforts are as effective and efficient as possible."
- NACCHO Developing a Local Health Department Strategic Plan: A How-To Guide
Striving for continuous improvement is a public health best practice, and evaluation of an assessment and planning process is a powerful method to apply it. Including evaluation into your CHAPS process will open up opportunities for further investment in quality improvement, performance management, and strategic planning. Although these are not requirements of the 2008 Colorado Public Health Act, they are key requirements of the PHAB accreditation process and are meant to improve public health programs, policies, processes, and interventions.
The final plan products will be based on both internal and external stakeholder needs. Traditionally, a single PHIP was produced but to keep these plans dynamic, effective, and working documents, they need to be accessible in a variety of different forms to meet the uses and needs of different stakeholders.
Components
A plan format is not required, however, here are important components you will want to consider including:
- Intro and orientation to purpose, content
- Description of jurisdiction: community profile, community vision, and values (this may also be part of the community health assessment or community health status report)
- Description of how all stakeholders involved developed the plan (community health assessment process, community engagement, prioritization process, development of goals, strategies, etc.)
- Capacity and performance assessment results
- Description of how stakeholders identified issues and needs
- Document process used to determine priorities
- Summary of priority areas, including why these were chosen and how your plan aligns with the state priorities:
- Data indicators and trends
- Goals
- Measurable objectives
- Improvement strategies
- Action steps with identification of lead agency or agencies and partners
- Evaluation and equity measures
- Financial resources available/required
- Plan for monitoring
- Plan for evaluation
- Acknowledgments
- Local board of health approval
- Where stakeholders can access plan and more information
LPHAs or partnerships that have not developed separate community health assessment reports are encouraged to include health assessment data in the PHIP. At a minimum, assessment data should be included in the summary of priority areas.
Format
Consider what formats are most likely to be used by the intended audience. For internal stakeholders, this includes what formats can allow you to easily revise and update the action steps in years two to five, as needed. Potential options include:
- Data dashboard
- Agency/partnership/partner website(s)
- Video
- Infographic
- Fact sheets
- Report
- Executive summary of key findings
- PDF for print as needed and electronic dissemination
- PowerPoint slides
- Hard copy, bound publication
- Hybrid, a mixture of some or all of the above
Discuss the merits and limitations of various formats and methods and decide what works best for your community. Regardless of the format(s) you choose, be consistent and systematic with documenting the processes, methods, and data sources. This will make it easier to monitor, refresh, evaluate, and replicate your assessment and plan.
The Colorado Public Health Act requires that the local PHIP be submitted to both the local board of health and the state Board of Health. Ideally, you will have engaged your board of health (BOH) throughout the CHAPS process, allowing them to provide feedback and direction and to be advocates for potential priority areas that have been identified in your public health improvement plan.
The following Local Board of Health Approval Guide & Fillable Form provides more detail on the acceptable documentation for board of health approval. The second page of this form is a fillable template that you may use to provide proof of LBOH approval. Just click the "download" button in the top right for a fillable PDF version of the form.
Upon review and approval from the BOH:
- Post on your agency and/or partnership website
- Submit your completed public health improvement plan and website link to OPHP via the following Google Form: click here to access the Google Form upload.
- Include documentation of BOH discussion/approval or a copy of meeting minutes/agenda. If you are submitting a plan as a partnership, the local board of health for each LPHA in the partnership will need to approve the plan individually.
- If you have any questions about submitting your plan online, contact us at ophp@state.co.us
OPHP will review each plan to ensure that it meets act requirements and present it to the state Board of Health for review. The Office also analyzes and summarizes each plan to inform the statewide public health improvement plan and to share with other local public health agencies, CDPHE programs, and other stakeholders.
How you communicate about the plan will impact how it is implemented and how impactful you can be.
Change the narrative
The community health improvement plan provides an opportunity to choose how you describe public health issues in new ways that connect social, environmental, political, and economic inequities to public and environmental health. This is especially important as Colorado's public health system moves towards addressing issues that are considered upstream or root causes to your communities' health and environmental issues.
Recommended communication resources:
- Office of Health Equity, Framing Data to Advance Health Equity tool
- FrameWorks Institute communication recommendations
- County Health Rankings &, Roadmaps communication guidance and tools
A communication plan may include:
- Update of your CHA communications plan
- Target audience(s) for the findings of your community health assessment, such as:
- Community members
- Partner agencies
- Local Board of Health
- Local Leadership
- Stakeholders identifying priorities for improvement plan
- How much, what kind, and what level of data is most useful for your audience(s)
- Data collection framework you chose to use when collecting data and a discussion about the best way to present the data to your stakeholders
- Next steps in the process and potential opportunities for engagement
Your communication process should include the following practices and activities:
- Use plain language by incorporating health literacy principles and plain language communication tools.
- Craft culturally and linguistically appropriate messaging, methods, and channels.
- Use emerging communication recommendations from resources like the FrameWorks Institute to articulate complex health issues in ways that resonate with your audiences and can lead to action.
- Test your communication messages and materials with a variety of audiences to ensure your community's health story is understood and is relatable.
- Use principles of community engagement to inform how you craft your communications and when to employ them.
- Use this step as a tool to model the changes you are aiming to make in the ways that you. How public health describes the connections between health issues and the underlying racial, social, and historical inequities can be a powerful strategy in and of itself.
- Discuss the merits and limitations of various communication formats and methods and decide what works best for your community.
Potential audiences may include:
- Those engaged during the assessment
- Leaders in positions of authority, such as the local board of health and/or county commissioners
- Potential local funders
- Key decision-makers in a position to make policy or systems changes
- Community partners that will help implement the plan
- Community members who will be impacted by the plan, if they have not already been involved
Examples for sharing out the PHIP that communities across Colorado have used include:
- Community open house
- Summit or conferences
- Presentations to local leadership or partners
- Email to community partners
- Posting on agency/partnership/partners website(s)
- Local artwork
- Press release(s)
- Paid/earned media
- Announcements via social media (Facebook, Twitter, etc.)
Regardless of the communication method(s) you choose, be consistent and systematic with documenting so that the effort can be monitored, refreshed, and replicated.
Phase 7: Implement, promote, and monitor
Use this phase to implement the Community Health Improvement Plan (CHIP) that you developed in Phase 6. A working CHIP that is monitored, evaluated, updated, and communicated to stakeholders on a regular basis will have the greatest success in improving the selected priority areas in your community.
Additional and external tools and guidance:
Responsibility
Determine the entity(ies) responsible for ensuring that the CHAPS process stays on track. This includes implementing the action plan(s) as well as continuing to coordinate the overall process, including monitoring, evaluation, and communication. Options to accomplish this includes re-directing the role and responsibilities of the advisory committee, designating priority area leads, or empower the internal agency staff to lead and coordinate accordingly with partners. Regardless of who is responsible, changes should be made in partnership with stakeholders through an agreed-upon process.
Questions to consider:
- Is there anyone missing from the advisory group with either content area knowledge or expertise in evaluation?
- What are your expectations from the leaders of the committees in terms of commitment and coordination?
- What kind of agreement would be most helpful in solidifying participation or financial commitment from partners? (e.g. MOU, IGA, contract, informal agreement)
- Are agency, community, and partnership members represented equitably?
- What are the expected outputs from implementation, evaluation, and monitoring activities? (e.g., evaluation plan, reports, etc.)
- What measures or processes will you put in place to ensure accountability and monitor the progress of the plan?
Stakeholder engagement
It can be challenging to keep stakeholders and partners engaged in the implementation of the plan. Involving a broad array of partners in specific monitoring and communication activities helps sustain their participation and the overall momentum of the process. Monitoring and evaluation efforts also can be used to:
- Improve program effectiveness
- Strengthen funding applications
- Increase political support
- Engage community residents
- Improve future assessment and planning processes
- Celebrate your successes
As you delve into the work outlined in your action plans, you will need to monitor and revise the content of your action plans at regular intervals. Use the process you developed in Phase 6, Step 6 to keep your action plans accountable, current and responsive to internal and external factors.
Updates will need to be made when an objective is completed, a new priority is identified, or a change in circumstances affects previous planning. Changes should be made in partnership with stakeholders through an agreed-upon process.
Review and make any necessary enhancements to your action plan(s) to ensure:
- Strategies and action plans mirror the actual work being done
- Adaptations are made based on action plan revisions and evaluation results
- Realistic and measurable objectives are related to each strategy
- Responsible individuals/organizations are identified as leads
- Appropriate people and organizations are included for each strategy. If they are not already participating, make plans to recruit them.
- Realistic timelines are set for each strategy
- Necessary and available resources have been identified
An ideal time to evaluate CHAPS is when you wrap up one cycle and prepare for the next.
Question(s):
During the development of the public health improvement plan (Phase 6), you and the advisory group will have outlined potential areas to evaluate, such as:
- goals and objectives determined in the action plan(s)
- process or outcome measures/indicators identified in the action plan(s)
- implementation of strategies (intended and unintended outcomes)
- community engagement throughout the process from data collection through implementation (satisfaction, inclusivity, quality, reach, etc.)
- partnership engagement throughout the process (satisfaction, inclusivity, geography, sectors, quality, reach, etc.)
- public health improvement planning process
- capacity to address health inequities
- communication methods and reach
Evaluation design and resources
Based on what questions you need to answer, determine the optimal type of evaluation, such as a process or outcome evaluation. Check out the following recommendations along with tapping into stakeholder expertise to carry out this important step.
- Evaluate actions, County Health Rankings and Roadmaps Action Center
- Measuring Success: Evaluating Comprehensive Community Initiatives, Community Toolbox
- Program Evaluation for Public Health Programs: A Self-Study Guide, CDC
- Designing Program Evaluation To Advance Equity, CO Office of Health Equity
Many communities choose to establish a subcommittee to oversee the evaluation activities; including the people who manage or work on the activities and those affected by its implementation will increase the usefulness and credibility of the evaluation. Developing a plan for evaluation will also support PHAB requirements related to tracking progress on implementation of your public health improvement plan.
Whichever type of evaluation your choose, the process should help you answer the following questions within each area you have chosen to evaluate:
- Did we achieve the goals we set out to?
- What were the impacts of the plan?
- Was there an equity impact?
- What do stakeholders want to know?
- What went well?
- What were the challenges?
- What improvements should we make and how?
Use the results
Results from your evaluation of the overall CHAPS process can add value the next time you start the cycle. Evaluation results that demonstrate the impact of your improvement plan can be useful in revising action plans and communicating progress. This process can also support documenting what went well and what could be improved the next go-around.
By this point in your process, your communication plan can be a tool to report on your progress and/or process to the community. Build off of your work in Phase 3 (Step 8 - Communicate findings and next steps) and Phase 6 (Step 10: Communicate results and next steps).
Change the narrative
The community health improvement plan provides an opportunity to choose how you describe public health issues in new ways that connect social, environmental, political, and economic inequities to public and environmental health. This is especially important as Colorado's public health system moves towards addressing issues that are considered upstream or root causes to your communities' health and environmental issues. Think critically and creatively about the story that your assessment and plan is telling. Use the implementation phase to change the narrative around complex health issues, advance equity, and address social determinants of health.
Recommended communication resources:
- Office of Health Equity's Framing Data to Advance Health Equity tool
- FrameWorks Institute communication recommendations
- County Health Rankings &, Roadmaps communication guidance and tools
Communicate progress and evaluation results
Among your key messages to share should be findings and lessons learned from your monitoring and evaluation activities. These can be interim findings and preliminary interpretations regarding improvements, since outcomes may take time to occur. These talking points will be valuable when communicating to those who have funded or contributed resources to the process. Likewise, these messages will be important to share with your stakeholders to demonstrate how their contributions - time, perspective, connections, resources - have made a difference.
Communicating change
Depending on your priorities, strategies, and stakeholders involved, you may have a degree of change that you need to communicate. These plans may represent doing things differently, addressing chronic issues in new ways, and involve new and different partners. Lean on change management principles and tools to further hone your communication efforts to ensure that you are meeting your audiences where they are.
Communication as community engagement
When and how you choose to do this can create two-way conversations. To do this, tailor your message and method depending on your audience and purpose. Differentiate between internal and external communication, and develop products that are appropriate and useful for each audience and communication platform (email, website, social media, presentation, etc.) including:
- Data dashboard
- Agency/partnership/partner website(s)
- Video
- Infographic
- Fact sheets
- Report
- Executive summary of key findings
- PDF for print as needed and electronic dissemination
- PowerPoint slides
- Hard copy, bound publication
- Hybrid, a mixture of some or all of the above
Use frequent, ongoing, and creative communication approaches to celebrate successes and recognize the hard work of participants and the efforts of the community. This is a multi-year project that you and your stakeholders will have endured together.
Phase 8: Participate in statewide public health improvement opportunities
Use this phase to connect local and statewide public health improvement efforts. Both local and state level public health entities are required to carry out public health improvement processes and follow the CHAPS process. This coordination enables local participation in the statewide planning process to inform data collection, issue prioritization, strategy identification and plan implementation and evaluation.
Use OPHP networking calls and peer-learning opportunities to share out your local public health improvement process, progress, and impact. CHAPS is co-developed and sustained by local and state public health practitioners.
Share with CHAPS users
- Report out on progress to OPHP. Phase 7 of CHAPS describes the process for regularly updating local public health improvement plans. OPHP is interested in receiving updated plans, including action plans, evaluation plans, communication plans and other related materials, to continuously improve Colorado's assessment and planning efforts and to share models with other agencies.
Share with the public health system
- Collaborate and network with other counties and partners on implementation efforts by sharing promising practices, collaborating on joint efforts, providing peer support, and networking. OPHP sponsors networking opportunities such as conference calls, webinars, and in-person meetings on a variety of topics.
The Public Health Act of 2008 also requires CDPHE to develop a state health improvement plan (SHIP.) Similar to local plans, this should be based on a comprehensive state health assessment every five years and is used to set priorities for the public health system.
The act identifies the need to incorporate, to the extent possible, goals and priorities of public health improvement plans developed by county or district public health agencies. It also requires plans to address how local public health agencies coordinate with CDPHE and others to accomplish goals identified in the SHIP. The Public Health Accreditation Board also requires alignment between the state health improvement plan and tribal, local, and national priorities as does Healthy People 2030.
Through CHAPS, local and state public health assessments and improvement plans and implementation can be coordinated to
- share data collection (qualitative and quantitative) results
- reduce burden of data collection on targeted communities
- inform each other's prioritization processes
- identify and elevate shared priority areas
- share and scale strategies to greater impact
- partner in the implementation of local and state plans, especially when strategies involve a variety of stakeholder levels
- inform monitoring and evaluation efforts to assess the effectiveness and impact of local and state processes
The priorities and objectives outlined in the state plan are intended to provide support, guidance, and focus for public health activities throughout the state. This coordinated state and local process enables enhanced management of resources, increased readiness for public health agency accreditation, and a more efficient approach to improving health outcomes.
Stay connected with OPHP to learn about opportunities to participate.