A1. Assessment and Planning

Assessment and Planning: Colorado’s governmental public health system will apply the principles and skilled practice of epidemiology, laboratory investigation, surveillance and program evaluation to support planning, policy and decision making in Colorado.
The public health system will monitor, diagnose and investigate health problems and hazards in communities including public health emergencies, outbreaks and epidemics, and collect and analyze data.
Links:
The source Core Public Health Services Operational Definitions Manual 2019 is organized as follows:
|
Functions of Assessment and Planning
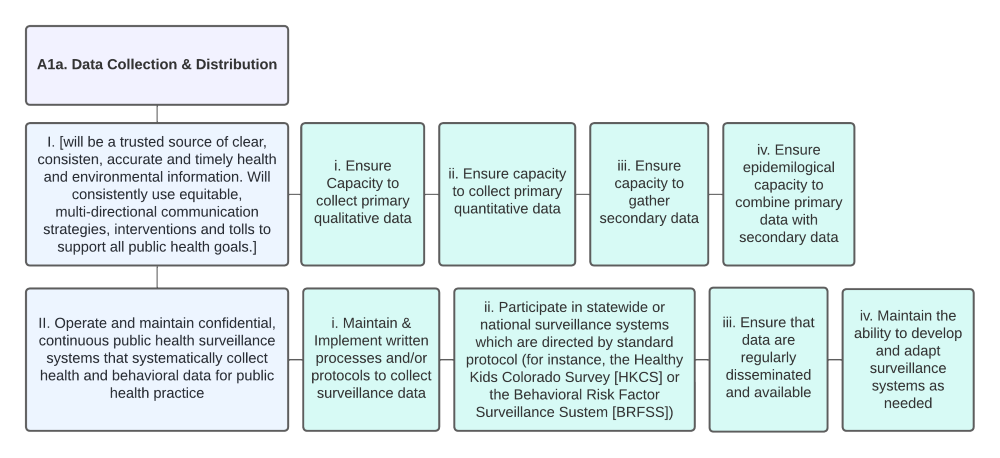
A1a. Data Collection and Distribution
I. Colorado’s governmental public health system will be a trusted source of clear, consistent, accurate and timely health and environmental information. The system will consistently use equitable, multi-directional communication strategies, interventions and tools to support all public health goals.
i. Ensure capacity to collect primary qualitative data.
ii. Ensure capacity to collect primary quantitative data.
iii. Ensure capacity to gather secondary data.
iv. Ensure epidemiological capacity to combine primary data with secondary data.
II. Operate and maintain confidential, continuous public health surveillance systems that systematically collect health and behavioral data for public health practice.
i. Maintain and implement written processes and/or protocols to collect surveillance data.
ii. Participate in statewide or national surveillance systems which are directed by standard protocol (for instance, the Healthy Kids Colorado Survey [HKCS] or the Behavioral Risk Factor Surveillance System [BRFSS])
iii. Ensure that data are regularly disseminated and available.
iv. Maintain the ability to develop and adapt surveillance systems as needed.
Related Links:
- American Community Survey (ACS) (US Census data)
- Colorado Health Access Survey (Colorado Health Institute)
- Colorado Health Indicators (CDPHE)
- Colorado Health Information Dataset (CoHID) (CDPHE)
- Colorado State Resources (County Health Rankings & Roadmaps)
- Environmental Public Health Tracking & EnviroScreen (CDPHE)
- VISION: Visual Information System for Identifying Opportunities and Needs (CDPHE)
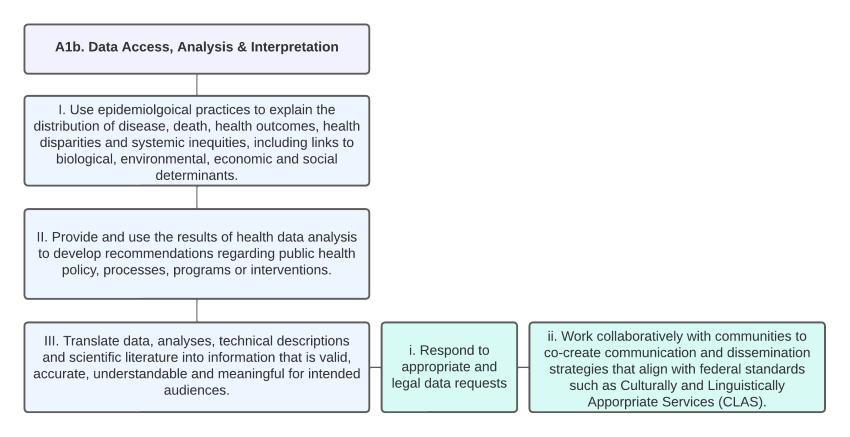
A1b. Data Access, Analysis and Interpretation
I. Use epidemiological practices to explain the distribution of disease, death, health outcomes, health disparities and systemic inequities, including links to biological, environmental, economic and social determinants.
II. Provide and use the results of health data analysis to develop recommendations regarding public health policy, process, programs or interventions.
III. Translate data, analyses, technical descriptions and scientific literature into information that is valid, accurate, understandable and meaningful for intended audiences.
i. Respond to appropriate and legal data requests.
ii. Work collaboratively with communities to co-create communication and dissemination strategies that align with federal standards such as Culturally and Linguistically Appropriate Services (CLAS).
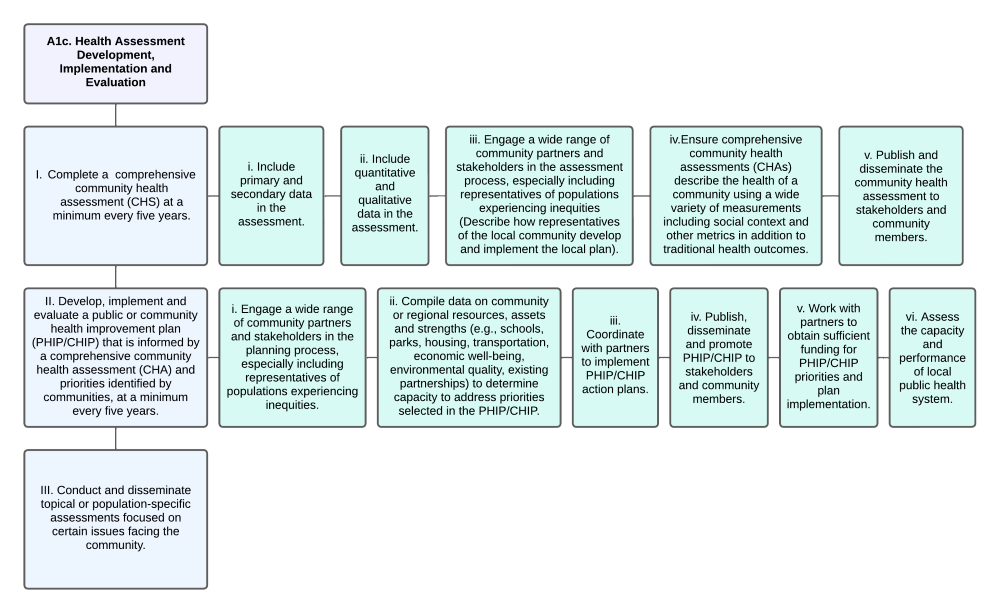
A1c. Health Assessment Development, Implementation and Evaluation
I. Complete a comprehensive community health assessment (CHS) at a minimum every five years.
i. Include primary and secondary data in the assessment.
ii. Include quantitative and qualitative data in the assessment.
iii. Engage a wide range of community partners and stakeholders in the assessment process, especially including representatives of populations experiencing inequities (Describe how representatives of the local community develop and implement the local plan).
iv. Ensure comprehensive community health assessments (CHAs) describe the health of a community using a wide variety of measurements including social context and other metrics in addition to traditional health outcomes.
v. Publish and disseminate the community health assessment to stakeholders and community members.
II. Develop, implement and evaluate a public or community health improvement plan (PHIP/CHIP) that is informed by a comprehensive community health assessment (CHA) and priorities identified by communities, at a minimum every five years.
i. Engage a wide range of community partners and stakeholders in the planning process, especially including representatives of populations experiencing inequities.
ii. Compile data on community or regional resources, assets and strengths (e.g., schools, parks, housing, transportation, economic well-being, environmental quality, existing partnerships) to determine capacity to address priorities selected in the PHIP/CHIP.
iii. Coordinate with partners to implement PHIP/CHIP action plans.
iv. Publish, disseminate and promote PHIP/CHIP to stakeholders and community members.
v. Work with partners to obtain sufficient funding for PHIP/CHIP priorities and plan implementation.
vi. Assess the capacity and performance of local public health system.
III. Conduct and disseminate topical or population-specific assessments focused on certain issues facing the community.
A1d. Vital Records
I. Record and report vital events (e.g., births and deaths) and act as the local registrar of vital statistics or ensure provision of the responsibility of registrar for each jurisdiction.
i. Collect, compile and tabulate reports of marriages, dissolutions of marriage and declarations of invalidity of marriage; births, deaths and morbidity; and require any person having information, with regard to the same, to make such reports and submit such information as is required by law or the rules of the State Board of Health.
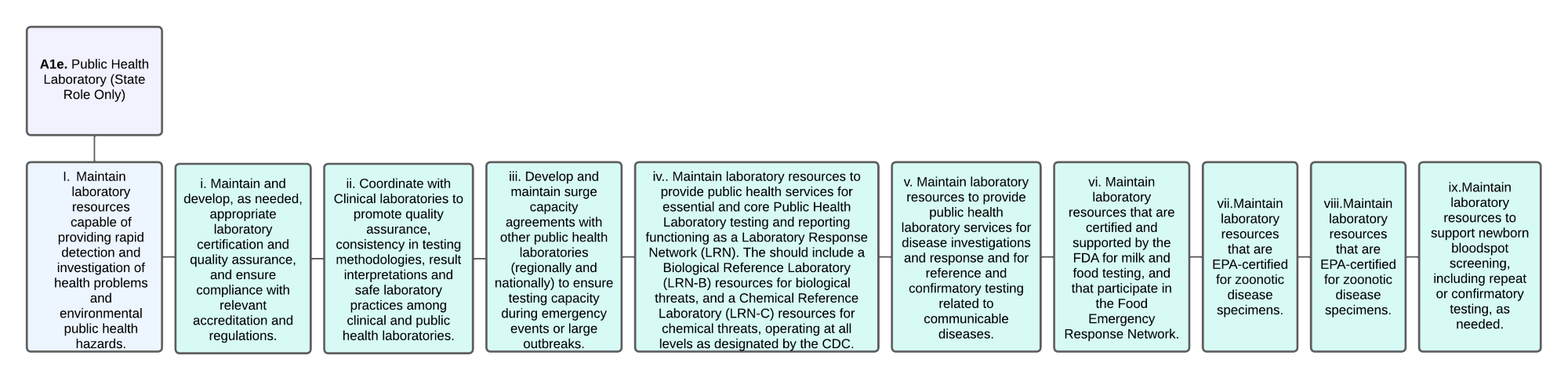
A1e. Public Health Laboratory (State Role Only)
I. Maintain laboratory resources capable of providing rapid detection and investigation of health problems and environmental public health hazards.
i. Maintain and develop, as needed, appropriate laboratory certification and quality assurance, and ensure compliance with relevant accreditation and regulations.
ii. Coordinate with Clinical laboratories to promote quality assurance, consistency in testing methodologies, result interpretations and safe laboratory practices among clinical and public health laboratories.
iii. Develop and maintain surge capacity agreements with other public health laboratories (regionally and nationally) to ensure testing capacity during emergency events or large outbreaks.
iv. Maintain laboratory resources to provide public health services for essential and core Public Health Laboratory testing and reporting functioning as a Laboratory Response Network (LRN). The should include a Biological Reference Laboratory (LRN-B) resources for biological threats, and a Chemical Reference Laboratory (LRN-C) resources for chemical threats, operating at all levels as designated by the CDC.
v. Maintain laboratory resources to provide public health laboratory services for disease investigations and response and for reference and confirmatory testing related to communicable diseases.
vi. Maintain laboratory resources that are certified and supported by the FDA for milk and food testing, and that participate in the Food Emergency Response Network.
vii. Maintain laboratory resources that are EPA-certified for zoonotic disease specimens.
viii. Maintain laboratory resources that are EPA-certified for zoonotic disease specimens.
ix. Maintain laboratory resources to support newborn bloodspot screening, including repeat or confirmatory testing, as needed.